Time for action: Advancing human rights for older Ontarians
Executive Summary
Time For Action: Advancing the Rights of Older Persons in Ontario is the final Report on the Ontario Human Rights Commission’s extensive research and consultation on human rights issues facing older Ontarians.
Currently, there are approximately 1.5 million older persons in Ontario. By the year 2021, Ontario will be home to three million people over the age of 65. As revealed in this Report, this significant and growing proportion of our province’s population faces significant barriers because of ageism and age-based discrimination. There is an urgent need for action to eliminate ageism and age discrimination so that older persons can fully participate in our communities, enjoy the same rights afforded to others and can live their later years with dignity. A new approach to aging is needed, one that promotes the dignity and worth of older persons and ensures their independence, security, full-participation and self-fulfillment.
The Report presents an overview of what the Commission heard from over 100 organizations and individuals from across the province. It outlines recommendations for government and community action derived from the suggestions of the consultees, as well as “Commission Commitments”, - steps that the Commission will take toward eliminating ageism and age discrimination in the province of Ontario.
Dignity, Independence, Participation, Fairness & Security
Dignity, independence, participation, fairness and security are identified throughout the Report as guiding principles central to any consideration of the issues related to older persons. These principles mirror the words of the preamble to the Ontario Human Rights Code and reflect the intent of its human rights protections. The Report highlights that these principles will be used in the Commission’s upcoming policy work on aging and it recommends that private and public sector organizations integrate these principles into their policies and programs.
Ageism
Ageism can give rise to individual acts of discrimination, but can also have a broader impact on policies, programs and legislation that affect large sectors of society. The Report identifies that barriers faced by older persons are often “socially constructed”, that is, they are not a direct result of the aging process but rather the result of society’s response to aging. It highlights that negative stereotypes and assumptions, failing to respond to the needs of older persons and, to design systems and structures that are inclusive of older persons are forms of ageism.
The Report’s recommendations emphasize the need to evaluate policies and programs to ensure they do not rely on or promote age-based stereotypes, as well as the need for education at all levels aimed at creating a positive perception of, and supportive environment for, older persons. It also outlines that the Commission will develop and implement a broad public awareness campaign that addresses ageism and age discrimination.
Age & Intersectionality
The Report highlights the unique and compound effect of aging on certain groups such as older women, older persons with disabilities, gay and lesbian older persons and older persons from diverse linguistic, religious, ethnic or racial backgrounds. It makes recommendations for community and government partners aimed at helping them to ensure that their policies and programs will not result in marginalization, disadvantage and discrimination for these particular groups.
Employment
Employment is fundamental to equal participation and opportunity in society and is central to a person’s sense of dignity and self-worth. The Report identifies age discrimination in employment, particularly in the form of mandatory retirement, and negative assumptions and stereotypes about older workers, as a serious concern. The Report describes experiences of age-based discrimination in the workplace, resulting in financial hardship, psychological and emotional distress and a sense of loss and outrage.
The Report emphasizes that mandatory retirement is discriminatory. It recommends that the Ontario Human Rights Code be amended to eliminate the defence of mandatory retirement at age 65 and to provide protections against age discrimination to workers over 65. Additionally, it asks employers to ensure that workplaces are free of ageist stereotypes, provide for equal opportunity and that workplace policies and procedures do not have an adverse effect on older workers. Finally, the Report highlights that the Commission will engage in public awareness activities to educate employers and employees about their rights and responsibilities under the Code and to encourage positive employment environments for older workers.
Housing
Affordable and accessible housing and the ability to age in one’s chosen surroundings are crucial to quality of life of older persons. The inadequacy of current affordable and accessible housing options, and the lack of social housing available in Ontario is discussed in detail throughout the Report. Additionally, the principle of “aging in place” is highlighted as a central concept with respect to housing options for older persons. Accordingly, the Report recommends that all levels of government cooperate to develop a strategy for affordable housing for older persons; ensure that the social housing supply in Ontario meets the current and future needs of older persons and other vulnerable persons in Ontario; that the provincial government amend the Building Code Act, 1992 to incorporate the best principles of barrier-free design; and that developers and builders design and implement barrier-free housing. It also highlights that the Commission will address the human rights issues facing older persons in its upcoming work on housing and human rights.
Health Care, Institutions & Services
Barriers to health care, institutions and services serve to adversely affect the dignity, self-worth, independence and full-participation of older persons. A number of barriers in the current health care system are discussed throughout the Report including the insufficient funding and resulting inadequacy of community-based care, the shortage of care professionals, and health care related costs. Physical barriers such as building accessibility and social barriers, such as restrictive attitudes within the health care system, are also addressed. Additionally, barriers in general services, particularly those in the area of transportation services, are highlighted.
Accordingly, the Report recommends that health care institutions, facilities and services be made accessible to all older persons, particularly those with disabilities; that the provincial government take further steps to regulate rest and retirement homes; and that medical schools and other health-related training centres take steps to ensure that graduates receive appropriate levels of training on the needs of older persons. In addition, it highlights that the Commission will work with faculties of medicine and other programs that educate professionals who work with older persons, to ensure that education on ageism and age discrimination is included within their curricula and will continue to work with service providers to promote accessibility throughout the province.
Elder Abuse
Elder abuse is a human rights issue requiring an effective and strong response by governments and communities throughout Ontario. The Report outlines the many forms of elder abuse and discusses ageism, social and economic vulnerability, caregiver stress, lack of regulation in care facilities, the shortage of long-term care beds, and inadequate accessible and affordable housing as contributors to elder abuse.
The Report recommends that mechanisms currently in place to address other forms of familial abuse be extended to apply to elder abuse and that provincial and municipal governments take steps to support specialized programs, including shelters, for victims of elder abuse. The Report also highlights that the Commission will continue to monitor the outcomes of the Round Table for Ontario’s Elder Abuse Strategy.
Elder Care
Elder care is a growing need requiring creative responses by government. Caregivers, largely female, are fulfilling an important societal role and should not have to bear the responsibility alone. The Report highlights that legislation, programming and funding as well as a commitment by employers to workplace flexibility are required to ensure that caregivers are supported as they balance the demands of care and employment.
On this basis, the Report recommends that the Ministry of Labour extend the new leave provisions of the Employment Standards Act, 2000, to smaller workplaces (including those of less than fifty employees) and that all levels of government and employers consider providing various forms of support to caregivers in the workplace. It also highlights that the Commission will engage in further work on the issue of elder care and will hear complaints from employees, who face discrimination on the basis of "family status", "marital status" and "same-sex partnership status" as they care for aging or ailing parents, spouses or same-sex partners
Conclusion
The issues identified in this Report raise significant human rights concerns to which the Commission and broader society must respond. The Commission is committed to working with government and community partners to ensure that these and future actions will afford older persons in this province a life free of discrimination and one full of dignity, independence, participation, fairness and security. It is with this in mind that the Commission respectfully sets forth this Report for consideration by all Ontarians.
| Attachment | Size |
|---|---|
| 283.78 KB |
Introduction
“...in a world of entitlements, we need to ask ourselves what we, as Ontario citizens, should expect to receive when we become older [and] what our older citizens should be receiving now.”
(Chatham-Kent Community Care Access Centre)
In 1999, the International Year of the Older Person, the Ontario Human Rights Commission (the Commission) began a study of the human rights landscape facing older Ontarians. The first step involved researching the main issues. The result was a Discussion Paper Discrimination and Age: Human Rights Issues Facing Older Persons in Ontario, released in July 2000. The Discussion Paper identified a number of issues that appeared to be of public interest. These were set out in further documents including a paper entitled The Changing Face of Ontario: Discrimination and our Aging Population which was issued in September 2000 and which began a process of extensive, province-wide consultation.
Information about the consultation process was sent to more than 400 stakeholders, posted on the Commission’s web site and advertised in newspapers. We received written comments from over 100 consultees. A Commission panel, chaired by Chief Commissioner Keith Norton, held public consultation sessions in London, Toronto, Ottawa and Sudbury. This Report is the culmination of our research and consultation. We are grateful to everyone who took the time to attend the public consultation sessions, to phone or to write to us as we have benefited greatly from their detailed and considered submissions.
The tremendous response we have received demonstrates the importance of this issue to all Ontarians. What has been made clear during this process is that our current approach to aging is not sustainable, especially given that by the year 2021, Ontario will be home to three million seniors, twice as many as in 1998. As a society, we can no longer afford to treat age discrimination as anything but a serious affront to the dignity and worth of the persons who experience it. A new approach is needed; one that promotes the dignity and worth of older Ontarians and allows for independence, security, full participation and fairness. We should ensure that we are treating today’s older adults in the way in which each of us would like to be treated when we become older. Now is the time for action: a change in attitudes, policies and practices must take place or Ontarians of all ages will feel the impact. The Commission hopes that this document articulates a vision for action and will be a starting point for change.
The scope of the report
This Report is intended to be a broad examination of all issues that may have an impact on the dignity and worth of older adults and that may affect the enjoyment of equal rights and opportunities.
The Commission’s mandate is set out in the Ontario Human Rights Code (the “Code”), the Ontario law that prohibits discrimination and harassment in five social areas: (1) employment, (2) housing, (3) goods, services and facilities, (4) contracts and (5) membership in trade, professional and vocational associations. The Preamble to the Code eloquently sets out its aim:
WHEREAS recognition of the inherent dignity and equal and inalienable rights of all members of the human family is the foundation of freedom, justice and peace in the world and is in accord with the Universal Declaration of Human Rights as proclaimed by the United Nations;
AND WHEREAS it is public policy in Ontario to recognize the dignity and worth of every person and to provide for equal rights and opportunities without discrimination that is contrary to law, and having as its aim the creation of a climate of understanding and mutual respect for the dignity and worth of each person so that each person feels a part of the community and able to contribute fully to the development and well-being of the community and the Province...
The Commission fulfills its mandate and strives to achieve the goals set out in the Preamble to the Code in two main ways: through receipt and enforcement of human rights complaints and by forwarding human rights policy and conducting human rights education. With respect to the policy and education function, the Commission is specifically empowered to:
- forward human rights policy;
- promote an understanding, acceptance of and compliance with the Code;
- provide public information, education and research aimed at eliminating discrimination;
- examine and review statutes, regulations, programs and policies and make recommendations on any provision, programs or policy that may be inconsistent with the Code;
- initiate investigations into problems and encourage and co-ordinate plans, programs and activities to reduce or prevent such problems; and
- encourage public and private organizations to undertake programs to alleviate discrimination (Section 29 of the Code).
It is pursuant to these powers that the Commission has undertaken this review.
This Report is intended to be a broad examination of issues that have an impact on the dignity and worth of older adults and that may affect the enjoyment of equal rights and opportunities.
The Report begins by identifying the need to consider dignity, independence, participation, fairness and security as core values in any consideration of issues related to older persons. In addition, it introduces the concept of ageism and its central role in age-based discrimination. The Report provides an overview of the particular disadvantage experienced by certain groups of older persons, based on the intersection of age with other aspects of their identity. Finally, the Report describes in depth what the Commission heard during its consultations with respect to employment, housing, health care, institutions and services, elder abuse and neglect and elder care.
This document will form the basis for future policy work by the Commission. The Commission’s policy statements provide information about the Commission’s interpretation of specific provisions of the Code. They are important because the public has the right to expect that the Commission will deal with cases in a way that is consistent with its published policies. They also set standards for how individuals, employers, service providers and policy makers should act to ensure equality for all Ontarians.
While the Commission intends to act swiftly on the commitments in this Report to do further work to promote the rights of older Ontarians, it is clear that action by the Commission is not enough. A concerted effort by all levels of government, the private sector, the non-profit sector and particularly those who work directly with older adults is needed. Policy and law-makers across the province must take steps to ensure equality for older Ontarians.
Accordingly, the Report makes recommendations for what others can do to address the practices and attitudes that limit the ability of older persons to participate fully in society. The submissions provided the Commission with a great number of recommendations for the manner in which age discrimination can be addressed. The Recommendations for Government & Community Action presented in each section of this Report are based on the suggestions received that particularly address the human rights issues inherent in age discrimination. They are intended to provide government and community partners throughout the province with suggested first steps through which they can work to combat age discrimination and its effects.
Additionally, each section outlines Commission Commitments which are steps that the Commission will take to combat age discrimination. The Commission looks forward to working with government, all sectors and community partners to encourage the implementation of the recommendations in this document.
A concerted effort by all levels of government, the private sector, the non-profit sector and particularly those who work directly with older adults is needed. Policy and law-makers across the province must take steps to ensure equality for older Ontarians.
Dignity, independence,participation, fairness & security
In the course of consultation, almost every individual and group highlighted the same central principles as requiring special consideration. These same principles have been identified in the work of national and international bodies. In particular, Canada’s National Framework on Aging[1], developed by the Federal, Provincial (with the exception of Quebec) and Territorial Ministers Responsible for Seniors to assist them in responding to the needs of a maturing Canadian population, recognizes the following five principles as most important:
“Much of human dignity is experienced and expressed through work. As social creatures we need to feel valued and empowered, feelings that come from knowing we are contributing to our social fabric...a significant number of people...experience feelings of uselessness and devalued self-worth upon retiring.” (Dee Stewart)
Dignity: Being treated with respect, regardless of the situation, and having a sense of self-esteem e.g., having a sense of self-worth; being accepted as one is, regardless of age, health status, etc.; being appreciated for life accomplishments; being respected for continuing role and contributions to family, friends, community and society; being treated as a worthy human being and a full member of society.
Independence: Being in control of one's life, being able to do as much for oneself as possible and making one's own choices e.g., decisions on daily matters; being responsible, to the extent possible and practical, for things that affect one; having freedom to make decisions about how one will live one's life; enjoying access to a support system that enables freedom of choice and self-determination.
“Affordable, accessible, flexible transportation is essential so clients can attend medical appointments in a comfortable and timely manner, achieve basic tasks, such as obtaining groceries, banking, other errands and decrease isolation by going on outings and seeing family and friends.” (KFL&A Community Care Access Centre)
Fairness: Having seniors’ real needs, in all their diversity, considered equally to those of other Canadians e.g., having equitable access (socially, economically, politically) to available resources and services; not being discriminated against on the basis of age; and being treated and dealt with in a way that maximizes the inclusion of seniors.
“We want not just to have things done to and for us, but to be full participants in the building and maintenance of a just and civil society.”
(Canadian Pensioners Concerned)
Participation: Getting involved, staying active and taking part in the community, being consulted and having one's views considered by government - e.g., being active in all facets of life (socially, economically, politically); having a meaningful role in daily affairs; enjoying what life has to offer; participating in available programs and services; and being involved and engaged in activities of daily living (decisions/initiatives in all spheres, not just those specifically oriented to seniors).
Security: Having adequate income as one ages and having access to a safe and supportive living environment e.g., financial security to meet daily needs; physical security (including living conditions, sense of protection from crime, etc.); access to family and friends; sense of close personal and social bonds; and support.
These principles mirror the words of the Preamble to the Code and reflect the intent of its human rights protections. They are therefore very relevant to, and will be used in, the Commission’s upcoming policy work on aging. In addition, these principles are useful beyond the confines of the Commission’s policy work. They can be applied broadly by government, the private and non-profit sectors and others in the development, analysis and evaluation of any new or existing policy or program that may affect older persons. The National Framework on Aging is a critical tool in this process. Recognizing the importance of such an analysis and this very important policy tool, the Commission recommends:
Recommendations for Government & Community Action
- THAT the five principles contained in the National Framework on Aging be integrated into policies and programs of public and private sector organizations.
[1] Canada’s National Framework on Aging is available from Health Canada, Health Promotion and Programs Branch, Division of Aging and Seniors and online: Health Canada <www.hc-sc.gc.ca/seniors-aines/nfa-cnv/>.
Ageism
During the consultation, the Commission heard repeatedly about ageism and its effects. Ageism can give rise to individual acts of discrimination, but can also have an impact on a wider scale by influencing policies, programs and legislation that affect broad sectors of society. For the purposes of this Report, the term ‘ageism’ refers to two types of behaviour that have a negative effect on older persons. The first involves the social construction of age, including incorrect assumptions and stereotypes about older persons. Another form of ageism involves a tendency to structure society based on an assumption that everyone is young, thereby failing to respond appropriately to the real needs of older persons.
Negative Attitudes and Stereotypes
The consultation emphasized that many barriers faced by older persons are attitudinal. Much of what we associate with aging is simply ‘socially constructed’. In other words, it is not a real component of aging, but rather society’s response to the process.
...the physical side of aging accounts for perhaps 25 percent of aging that we see in American society. Seventy-five per cent is accounted for by another type of aging which has no physical basis. It is the role which our folklore, prejudices, and misconceptions about age impose on “the old”.[2]
The Commission heard many examples of negative attitudes and stereotypes:
“...I was terminated after 24+ years of service at age 58 and was told that “anyone over 50 was unable to be trained.”
“There is a myth that at age 65 people suddenly become ill, demented, dependent and fold their hands and go on the dole.”
(Canadian Pensioners Concerned)“...there is a growing tendency to blame the elderly for... escalating health care costs and difficulties in accessing...services...[This] is often evident in how both the public and media frame discussions of health care issues... [There is a] pejorative labelling of older adults as ‘bed blockers’...” (Ontario Association of Social Workers)
“Stereotyping and negative attitudes... is the dominant theme that we see in the course of our work. We strongly agree that stereotypes about aging and ability of older persons give rise to discriminatory treatment.” (Advocacy Centre for the Elderly)
Perhaps one of the clearest examples of ageism is observed in the Code itself. The definition of age in section 10(1) states:
The restricted definition of age in human rights law, which allows employers to implement mandatory retirement at age 65, demonstrates how deeply ageism is ingrained in our culture.
“age” means an age that is eighteen years or more, except in subsection 5(1) where “age” means an age that is eighteen years or more and less than sixty-five years;
Section 5(1) prohibits discrimination in employment. This means that persons over the age of 65 cannot make a complaint of age discrimination in employment. This also allows employers to implement mandatory retirement at age 65 and prevents anyone from making a complaint that being forced to retire at 65 is discriminatory.
This restricted definition of age in the Code demonstrates how deeply ageism is ingrained in our culture. Some have noted that it also serves to perpetuate ageism as it sends a message that workers over 65 do not have the right to be free from age-based discrimination.
Ageism and its effects extend well beyond the issue of mandatory retirement. The Commission also heard that ageism contributes to elder abuse and plays a prominent role in the barriers to housing, health care, services and institutions. Consultees told the Commission that ageist assumptions can be found in the manner in which health care and service providers approach older persons and the way in which housing options are formulated for older persons in Ontario. In effect, ageism, in its various forms, serves to disempower older persons within these very important aspects of their lives.
Failing to Take the Needs of Older Ontarians Into Account
The Commission heard many examples of the second form of ageism, namely the failure to respond to the real needs of older persons and to design systems and services that are inclusive for older persons:
“Ageist attitudes persist with many physicians, e.g. “what do you expect for your age?” ...especially if there is a mental health problem.” (Canadian Mental Health Association – Windsor-Essex Branch)
- treating certain conditions such as hearing loss or depression as a ‘normal’ part of the aging process and, therefore, not providing appropriate assessment and treatment;
- timing traffic lights based on how long it would take a young person who has no disability to cross the street, instead of taking into account how long it might take an older person, especially someone with a disability, to safely make the crossing;
- focusing health care spending on acute care with insufficient emphasis on long-term, chronic care; and
- providing services with an emphasis on how quickly and ‘efficiently’ people can be served which may result in insufficient time being spent with older clients.
Our society should be structured and designed for inclusiveness. The needs of all citizens, including older persons, must be taken into account up-front so that physical, attitudinal and systemic barriers are not created. Assuming that everyone is young and able-bodied and designing programs and facilities on that basis is a form of ageism that must be addressed in our society. The Commission heard that some levels of government are now undertaking gender-based analysis. Similarly, government should consider the impact of laws, policies and programs on all age groups.
Measures to Combat Ageism
Acknowledging Contributions[3]
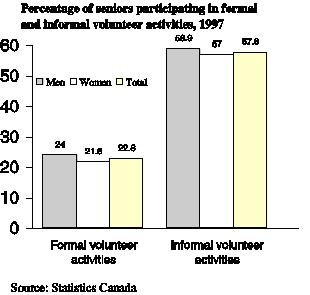
The Commission was told that more emphasis must be placed on the contributions made by older persons. They provide wisdom and experience, as illustrated by the fact that many judges and politicians are older persons, and many are entrepreneurs and employers. Older persons are consumers in the economy and investors; they also play a critical role as caregivers and volunteers. These contributions should be acknowledged through more positive portrayals of older persons.
As one group noted: “Consideration should also be given to the recognition of the part older persons can continue to play, not only as workers, volunteers and citizens...with a wealth of life experience, but also in the development of public policies which affect all people in communities” (Canadian Pensioners Concerned).
Public Awareness Campaigns and the Media
Participants told the Commission that there is a need for public awareness campaigns, using radio, television, print media and other means such as transit ads, to counteract myths and stereotypes about older persons. These campaigns should provide a positive portrayal of older persons by showing them as active and contributing to society. One group noted that these campaigns are not just to combat ageism but also to empower those experiencing ageism to recognize what it is and how to respond. In addition to using the media to raise awareness, it was suggested that there should be monitoring of the portrayal of older persons in the media to ensure that it is balanced and not contributing to negative attitudes.
Initiatives in the Education System
Participants stressed the importance of changing attitudes about older persons at an early age. As one group noted: “Attitudes are established at a young age. Negative images of older persons can generate a strong age bias early in life. Myths and stereotypes are developed. If left unchallenged, they become lifelong beliefs and ageism emerges” (United Generations Ontario).
“Our experience clearly shows that programs and activities that bring members of different generations together in meaningful ways breakdown stereotypes, destroy myths and create a climate of mutual caring and sharing.”
(United Generations Ontario)
Therefore, initiatives to raise awareness about ageism, in both its forms, and the aging process should be introduced into public and secondary schools. One group suggested that intergenerational programs can be particularly successful in breaking down barriers between the generations and combating ageism. An intergenerational program is a planned, intentional interaction of different age groups, infant to elderly, in a variety of situations at a level that provides close communication, sharing of feelings and ideas, and cooperative activity in meaningful tasks. Such programs can serve to promote health and well being not only for older persons but also for society as a whole.[4]
Many of the submissions focused on the need for educational initiatives in post-secondary education and in training for specific jobs. In particular, those who work with the public should receive training that dispels negative assumptions and attitudes and serves to increase awareness of how to appropriately respond to the aging process. Educational initiatives should include enhanced training in gerontology, care-giving skills, communications techniques and education with respect to cognitive deterioration caused by dementias (e.g., Alzheimer Disease). The Commission heard that improved training for doctors, nurses, other health care professionals, police, lawyers, journalists, social workers, policy-makers and others who work directly with older persons would be a starting point:
“The training of [public transit] employees should include age and disability awareness.” (Ontario Coalition of Senior Citizen’s Organizations)
“Special training needs to be provided to caregivers and to those who work in residential complexes for seniors.”
(Canadian Hearing Society)“With the aging of the population and longer life expectancies, physicians need to become more familiar with the aging process and the health needs of older adults. Currently, the five medical schools in Ontario allocate a minimal percentage of their medical school curriculum to aging or dementia...Since family physicians are often the first point of entry into the health care system, it is important that they receive more in-depth training than is currently offered.” (Alzheimer Society of Ontario)
Consultees told the Commission that education must also be aimed at older persons so that they can identify if and when they are experiencing ageism or age discrimination and know what recourses are available to address it.
Additional Measures
Other suggested measures include:
- ongoing communication with the public, especially seniors groups, to identify and discuss ageism and how to combat it;
- province-wide distribution of educational materials on ageism and age discrimination, preferably in written and audiovisual formats;
- public education forums across the province;
- education on ageism in the workplace; and
- the review of all government laws, policies and programs using an “older age analysis” to see if they appropriately take the needs of older Ontarians into consideration.
The Commission is very concerned that ageism and age discrimination do not appear to invoke the same sense of moral outrage and condemnation as other forms of unequal treatment. Recognizing that ageism is ingrained in societal structures and attitudes and that it gives rise to discrimination against older adults the Commission recommends the following specific measures to combat both forms of ageism.
Recommendations for Government & Community Action
2. THAT all levels of government evaluate laws, policies and programs to ensure that they do not contain age-based assumptions and stereotypes and that they reflect the needs of older persons.
3. THAT the Ministry of Education, school boards and schools develop programs and activities that will encourage a better understanding and a more positive perception of older persons. Intergenerational programming between students and older persons is an integral part of such education.
4. THAT professional faculties such as medicine, nursing, social work and nutritional sciences should better prepare their graduates to work with older persons in a more supportive manner, without stereotypes and assumptions.
5. THAT regulated professions and voluntary professional associations take steps to raise awareness among their membership about ageism and age discrimination and provide continuing education in this area, for example through courses and publications.
2. Commission Commitments
1. The Commission will develop a public policy statement on age discrimination in 2001/2002.
2. The Commission will develop and implement a broad public awareness campaign that addresses ageism and age discrimination.
[2] A. Comfort, “Age Prejudice in America.” (1976) 7 Social Policy at 4 as cited in Dr. M. Shipman, “Intergenerational Programming from Instrumental Action to Social Imperative and a Vision of a Civic Society” (Research Commissioned by the Vanier Institute of the Family, August 1996) at 6.
[3] Percentage of Seniors Participating in Formal and Informal Volunteer Activities, 1997 from Health Canada, Division of Aging and Seniors, Statistical Snapshot No. 20: Giving Back to the Community, online: Health Canada, Division of Aging and Seniors <www.hc-sc.gc.ca/seniors-aines/pubs/factoids/en/factoid.htm>.
[4] For detailed information about intergenerational programming, see Shipman, supra, note 2.
Age & intersectionality
The Commission recognizes that persons may experience disadvantage in unique ways based on the intersection of age with other aspects of their identity. During the consultations, the Commission heard about certain groups of older persons who face particular barriers arising from the intersection of age with gender, disability, sexual orientation, race, ethnicity, religion, culture and language.
“Women particularly suffer because of past customs, practices and traditions.” (Canadian Pensioners Concerned)
Age & Gender
While older men do experience particular concerns, many submissions emphasized the unique and often compounded disadvantage experienced by older women.
One of the most pressing concerns for older women relates to their socio-economic
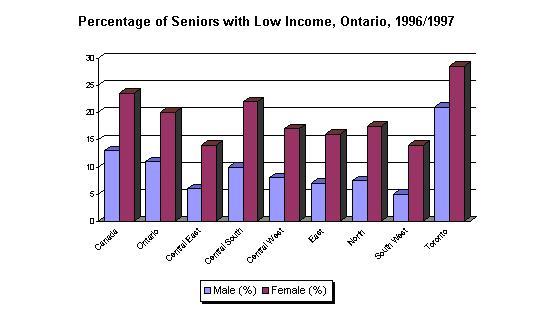
status. Owing to a number of factors including longer life expectancy, labour force participation patterns, wage inequality, social programs and systems designed primarily from a male-centred or gender-neutral perspective, older women are more likely to experience poverty. [5]
In addition, as noted by one organization “most elderly persons are women and the prevalence of women in the population increases with age. Among people over 65, 58 percent are women, while among those over 85, 75 percent are women” (Ontario Association of Social Workers). Therefore, women are disproportionately represented in the group of older persons who tend to be most vulnerable and in need of services and supports.
“There are particular problems for elderly women. In Ottawa-Carleton there are some 33,000 seniors aged 75 and older, according to the 1996 census, nearly two-thirds of which [sic] are women. Of these women, half had annual incomes of $16,000 or less, and half live alone. This, in our view, creates a vulnerable population to the problems of abuse and discrimination, and requires a more proactive response by government.” (Council on Aging – Ottawa-Carleton)
As a result of these factors, the issues that have been raised as a concern for older persons throughout the Report may be more acute for older women. The following areas tend to be of particular concern.
Health care, Home care and Institutions: Health care has been noted as one of the most pressing needs of older women. Older women are less likely than their male counterparts to rate their health as good, very good or excellent and more likely to rate their health status as fair or poor. Older women also average the longest hospital stays and with increasing age, more females than males need help with daily activities.[6] These and other statistics suggest that the concerns related to health care and home care identified in this Report may disproportionately affect women.
The majority of older persons live at home. However, among those who do live in institutions such as nursing homes, retirement homes and long-term care facilities, a larger number are older women. In 1996, 38% of all women age 85 and older lived in an institution compared to 24% of all men age 85 or more.[7] This means that issues concerning regulation of such facilities are of particular concern to older women.
“There is a growing risk of homelessness amongst older women”
(Older Women’s Network)
Housing and Community: The Commission was told that older women suffer due to a lack of affordable, suitable housing. Concerns were expressed with respect to the lack of rent control in the rental housing market, the physical inaccessibility of housing for older persons, the inadequacy of social housing and the need for options that allow for “aging in place”. Given that women have longer life expectancies, and are more likely to be widowed, many of the identified issues affect older women in a disproportionate manner.
Transportation: In order to access the services and supports they need and to participate in community life, affordable accessible public transportation is an important issue for older women.
Caregiving: Women make up the vast majority of paid and unpaid caregivers. The Commission was told that wives, sisters, daughters and daughters-in-law are providing most of the unpaid eldercare in the province. The devaluing and lack of societal support for the role of caregiver has a disproportionate impact on women of all ages.
Elder abuse: Freedom from abusive behaviour, including physical abuse, sexual abuse, emotional abuse, neglect or financial abuse, by family or professionals has also been identified as a significant concern. Both men and women are at risk for elder abuse and neglect. Because older women make up a higher proportion of the frail elderly, they are more likely to experience certain kinds of abuse. Older women are also more likely to experience abuse by their spouse than are older men. Women 65 years of age or more are more frequently the victims of violence at the hands of family members than are men.[8] Accordingly, issues regarding elder abuse are a concern for both male and female victims, although the particular vulnerability of women in the context of elder abuse must be recognised.
Employment: In the context of employment and pension benefits, many of the current systems were designed on the basis of a workforce that was primarily male and on the assumption that women were supported by male wage earners. As a result, women face unique and compounded disadvantage in the context of employment related-discrimination. In turn, mandatory retirement has a particularly harsh impact upon women. The section on Employment provides a thorough discussion of these issues.
Older Men
Many of the issues raised in this Report also concern men, and older men face their own unique issues.
Consultees said that the gendered division of labour experienced by many older persons means that older men may not be able to cope with their own personal needs upon the death of a partner or a family member who was responsible for household tasks such as cooking, laundry etc. In addition, the Commission heard that single older men who have lost their family caregiver seem to have difficulty in accessing community services. As the Commission heard:
“Single older men, who have lived most of their lives with a partner and are now living on their own are also a group needing specific support as most have never cooked, shopped, done laundry or managed other household chores.” (Dieticians of Canada)
“A gentleman who was receiving a lot of care at home by his wife...his wife had a fall in her home. She fell and ended up in a coma going to the hospital. He could not make his own meals, had an addiction problem and was basically isolated and alone in his home...He had no avenue to access services.” (Senior Link)
As well, high suicide rates exist among older men, particularly over the age of 85.[9]
Given what the Commission heard regarding the intersection of age and gender, the Commission recommends the following:
Recommendations for Government & Community Action
6. THAT government, the public and private sectors consider the ‘intersectional effect’ of age and gender in policies and programs, especially with respect to the compounded disadvantage experienced by older women.
Age & Disability
Many older persons are active, healthy and physically fit. Perceptions that older persons are weak and frail do not reflect the fact that the majority of persons over 65 consider themselves in good health.[10] Moreover, many older persons, who do have a chronic health condition or a disability, continue to lead fulfilling lives.
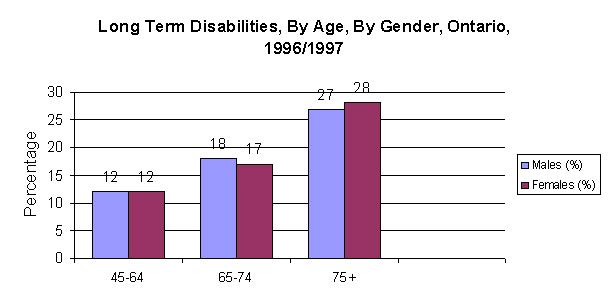
Nevertheless, it is important to acknowledge that with increasing age, the prevalence of disabilities and chronic conditions also increases. Recognition of this fact is necessary to ensure that appropriate supports and services will be put in place to meet the needs of an aging population. As discussed elsewhere in this Report, it also underscores the need for appropriate training in geriatrics, psycho-geriatrics and geriatric nursing for health care professionals and other service providers.
For persons with disabilities, aging can result in a disproportionate impact or unique experiences of discrimination. Moreover, multiple disabilities can create a ‘domino effect’.
For persons with disabilities, aging aggravates chronic patterns of poverty and social discrimination. When disabilities develop later in life, individuals can experience sudden and devastating changes in lifestyle and living standards. Aging can result in a disproportionate impact or unique experiences of discrimination. Moreover, multiple disabilities can create additional barriers and limitations on the ability to fully-participate in society. The Commission learned that where older adults are already experiencing isolation, for example, because they live in rural or northern areas, having a disability can compound the effect of the isolation. The following is a brief summary of some of the most important issues that relate to aging and disability.
Health care, Home care and Institutions: As discussed in the section on Health Care, Institutions and Services, there is a need to ensure that health care and home care services respond to disabilities associated with aging. Funding community-based care and long-term care at sufficient levels is one way to address this need. Health care providers also require appropriate training in disabilities associated with aging such as hearing loss and cognitive disabilities. Health care facilities and institutions should be designed to maximize safety, integration and comfort. They should be physically accessible (i.e. ramps, TTYs etc.) and services must be provided in a manner that accommodates disability related needs (i.e. sign-language interpretation).
Up-front barrier-free design promotes “aging in place” and is more cost effective than retrofitting inaccessible dwellings when a disability develops.
Housing: Housing should address disability-related needs associated with aging. Consultees told the Commission that housing design should address current needs and be flexible enough to accommodate future disabilities. This type of up-front, barrier-free design promotes “aging in place” and is more cost effective than retrofitting inaccessible dwellings when disability develops. Suggestions for design features that would respond appropriately to the needs of older persons with disabilities are discussed in section on Housing.
The Commission also learned that more specialized housing for Deaf, deafened and hard of hearing older persons and for others with particular disabilities is needed. As well, government involvement in the development of social housing for older persons with disabilities is required. Consultees told the Commission that Ontario requires housing that provides a continuum of care with the capacity to support the disability-related needs of older persons throughout the aging process. Finally, the Commission heard that the concept of “aging in place” is a critical housing principle for older persons with disabilities.
Transportation: Public transportation is critical for the independence and participation of older persons. In February 2000, the Commission released its Discussion Paper on Accessible Transit Services in Ontario.[11] The paper emphasizes that conventional transit systems must ensure maximum accessibility and that parallel para-transit services should be available for those who cannot access even the most integrated conventional system. During the consultation, consultees echoed the same concerns. Concerns were raised about narrow criteria for determining eligibility for para-transit services. Consultees offered suggestions for ways in which the accessibility of transit systems can be improved. A more detailed discussion of transportation issues appears in the section on Health Care, Institutions and Services.
“In the last number of years, there have been many governments and companies who have been down-sizing, and many deaf employees who are 45 years of age and older have been laid off their jobs. They may have been and often have been working in the same job for 10 or 20 years right after high school, and suddenly they are laid off. They haven't had an opportunity to upgrade their skills. They aren't prepared for today's job market.”
(Canadian Hearing Society – Ottawa)
Employment: A 1998 survey of approximately one thousand Deaf Canadians illustrates in statistical terms the particular disadvantages faced by older persons with disabilities in the employment context. The Employment and Employability of Deaf Canadians study reported that for the 52-64 age group, only 30% are employed while 27% are underemployed[12] and 43% are unemployed. Between ages 52-64, Deaf individuals experience an enormous 17% shift from employment to unemployment, a rate much higher than the national average of all Canadians.[13] This has been attributed to an obsolescence of skills rather than voluntary early retirement.[14]
In the context of employment, the Commission was told that older workers with disabilities may be more likely to lose their jobs in a workplace reorganization as a result of having had fewer opportunities to upgrade their skills or because of a perception that their disability makes them harder to place in a different job.
In addition, both age and disability are barriers for individuals when trying to get a job. Therefore, in the context of a labour market that favours youth, an older person with a disability may face additional hurdles to finding employment. As one group explained, prejudice based on age and disability amounts to “double-edged sword” for older persons (Canadian Hearing Society – London).
Additional Concern: The Building Code Act: The Commission was very concerned to learn that the standards for barrier-free design that are already contained in the Building Code Act, 1992[15] are often not met by builders or enforced by inspectors. For example, the Commission was told that the requirement in section 3.8.3.7 of O. Reg. 403/97 under the Building Code Act, 1992 that classrooms, auditoria, meeting rooms and theatres “shall be equipped with assistive listening systems” is rarely adhered to. The Building Code Act, 1992 itself could be improved by addressing additional elements of barrier-free design.
The Commission recently released its new Policy and Guidelines on Disability and the Duty to Accommodate.[16] The Policy sends a clear message that employers, landlords, service providers, and those who deliver programs are expected to take proactive measures to ensure that persons with disabilities can be equal participants in society. It emphasizes that the duty to accommodate is not optional and meeting the needs of persons with disabilities is a legal obligation up to the point of undue hardship. The Commission has confirmed that the undue hardship standard is a high one. As the Discussion Paper noted, these principles apply equally to older persons with disabilities.
Recommendations for Government & Community Action
7. THAT the provincial government enact legislation that will set minimum standards for accessibility for persons with disabilities, including older persons..
8.THAT government, the public and private sectors consider the ‘intersectional effect’ of age and disability in policies and programs, especially with respect to the compounded disadvantage experienced by older persons with disabilities.
“Older Gay and bisexual men and lesbians experience ageism within traditional gay spaces and homophobia within traditional ‘senior’ spaces.”
(AIDS Committee of Toronto)
Age & Sexual Orientation
The Commission heard about the exclusion of older gay men, lesbians and bisexual persons in the context of the gay community and broader society. As well, a number of concerns were identified regarding homophobia and discrimination in the context of employment and community-based care and long-term care facilities. The concerns regarding the intersection of homophobia and ageism that were emphasized, illustrated that in any future work in the area of elder abuse, an intersectional analysis that also takes into account sexual orientation will be critical.
“We have lesbian great-grandmothers, gay uncles, and bi-sexual cousins! Principally what has changed is the number of people prepared to come out and be publicly identified.”
(The Coalition of Lesbian and Gay Rights in Ontario)
The Commission heard that there is great emphasis placed on youth within the gay community, which can result in the marginalization of older gay men. The Commission was told that “most spaces and organizations are geared toward younger people” (AIDS Committee of Toronto (ACT)). There is a stereotype that gay, lesbian and bisexual persons are all young in age and it is often assumed that there were few or no gay men, lesbians and bisexuals in previous generations. This can translate into a failure to recognize the existence of older gay men, lesbian and bisexual persons and their partners and has serious implications for their experience in social areas such as services, health care and institutions. The Coalition of Lesbian and Gay Rights in Ontario (CLGRO) noted that “there are older lesbians, gays and bisexuals moving through the system now – in residential homes, using the healthcare system and social services available...many of them will not come out and the willful [sic] ignoring of their needs [and] the homophobia they witness can convince them that they were right not to.” Clearly these issues adversely impact an older person’s rights to dignity, full-participation in society, fairness and security.
Employment: One group noted that older gay men, lesbians and bisexual persons face the same barriers faced by other older workers, yet this burden is compounded by homophobia. The Commission was told, “older lesbians, gays and bisexuals are particularly prone to pressure to take early retirement schemes where employers do not want them in the workforce” (CLGRO). Homophobia in the workplace can make the option to leave, even if not favourable, attractive. Lesbian and bisexual women face the same economic disadvantage as heterosexual women given that women in general continue to earn less than men in the workforce. Where homophobic work environments create barriers to advancement, however the disadvantage experienced by lesbian and bisexual older women is intensified.
Elder Care: The increasing reliance upon family and friends to provide care for aging relatives may not be possible for some older gay men, lesbians and bisexual persons. ACT told the Commission that, “many older gays and lesbians do not enjoy the familial support that many heterosexual seniors can turn to in later life. They may have no family at all to turn to for emotional, financial or practical assistance and support.” Additionally, due to the impact of AIDS in the gay community, many older gay men have lost entire circles of friends, so the relationships they had developed to facilitate their older years are also gone. Our system of health and social services is based on traditional assumptions about family and social relationships that in fact may pose barriers for gay, lesbian and bisexual older persons.
Health Care, Institutions and Services: Homophobia in the health care system was identified as a prominent concern. The Commission was told by CLGRO that studies of systemic barriers to provincial health and social service systems have identified pervasive homophobia on all levels, resulting in situations from mild neglect to faulty medical treatment. ACT told the Commission that the homophobia that is directed at gay, lesbian and bisexual persons by the staff of care facilities, “is a frightening and realistic one for many older gays and lesbians...they fear homophobic violence, both physical and verbal/emotional.” In addition, health care professionals need to be more knowledgeable and sensitive to lesbian, gay and bisexual issues. In the area of community-based care, where volunteers may be relied on to provide care, education and regulation is particularly challenging yet needed.
“Older gay men are very concerned about where they will go when they can no longer be self-sufficient. They fear seniors’ residences and homes where their sexual identity and history will not be present, respected or validated. Older gay couples fear being split up at the end of their lives because there really is no space they can go that will respect them as a couple.”
(ACT)
In the context of residential homes for older persons, the Commission heard that gay, lesbian and bisexual partners are not always recognized. As one group stated, “we still have a struggle to get doctors, caregivers and other professionals to accept our partners as our spouses...something as simple as placing a photo of a spouse on the bedside table can bring about repercussions” (CLGRO). Older gay couples fear being split up at the end of their lives because of this prejudice. In addition, gay, lesbian and bisexual persons fear that their sexual identity and history will not be respected or validated in residential facilities.
Recommendations for Government & Community Action
9. THAT government, the public and private sectors consider the ‘intersectional effect’ of age and sexual orientation in policies and programs, especially with respect to the compounded disadvantage experienced by older gay, lesbian and bisexual persons.
10. THAT health care and social service providers receive training to enable them to appropriately address the needs of older gay, lesbian, bisexual and transgendered persons.
11. THAT residential facilities ensure that gay, lesbian, bisexual and transgendered residents are protected from homophobia, and afforded the same rights and recognition of their relationships as other residents.
Age & Citizenship Status, Religion, Language, Ethnicity, and Race
The intersection of age and citizenship status, religion, language and ethnicity has implications for health care, services and institutions:
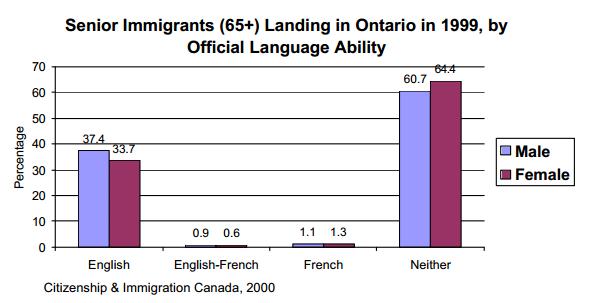
Health Care, Institutions and Services: The Commission heard that there is little recognition of the diversity within the population of older persons in Ontario. The Commission was told that a person’s immigration status in Canada can limit access to health care services. Participants noted that the provision of health care information in only French and English means that those who speak other languages may not receive critical information. Others noted that there is a shortage of French language services thereby further limiting access. In 1999, the largest percentage of immigrants to Ontario, age 65 and older, were not conversant either in English nor French:[17]
Additionally, 1996 Census Canada statistics note that of older Aboriginal persons in Ontario, 57.7% were conversant in English, 7.4% in French and 34.8% were conversant in non-official/aboriginal languages.[18] Together, these statistics illustrate the need for health care and other service providers to ensure that their services can be accessed by the variety of linguistic groups represented in this growing population older persons in Ontario.
Concerns were also expressed about the manner in which service providers currently address the needs of various groups of seniors within long-term care facilities. The provision of food, social and recreational activities in such institutions may not respond to the particular cultural and religious needs of some older persons. Service providers in all sectors must respect the identity and dignity of all persons and be sensitive to the diverse cultural and religious needs of older persons. This is equally important on the basis of race and ethnicity.
The Commission heard that there is a need for further consultation with older persons to discover the barriers faced on the basis of the intersection between age and ethnicity, citizenship, religion, race, and language.
Recommendations for Government & Community Action
12. THAT health care and other service providers should seek to find ways to deliver services to a range of ethnic, cultural, racial, linguistic and religious groups.
[5] Statistics Canada, Percentage of Seniors with Low Income, Ontario, 1996/97 from Third Age Ontario Intranet, online: <www.mczcr.gov.on.ca/thirdage/>.
[6] Ibid. and Health Canada, Division of Aging and Seniors, Statistical Snapshot No. 47: Hospitalization of Seniors supra, note 3.
[7] Health Canada, Division of Aging and Seniors, Statistical Snapshot No. 12: Institutional Living, supra, note 3.
[8] Statistics Canada, Family Violence in Canada: A Statistical Profile (Ottawa: Minster of Industry, June 1999) at 23-4.
[9] From Third Age Ontario Intranet Web site, supra note 5.
[10] Statistics Canada, Self-Rated Health of People 65+ and 75+, by Gender, Ontario from Third Age Ontario Intranet Web site, supra note 5.
[11] Ontario Human Rights Commission, Discussion Paper on Accessible Transit Services in Ontario (February 2001) available online at www.ohrc.on.ca.
[12] The term “underemployed” is used to describe people who may not be satisfied with their current job, may have experienced job insecurity, or may face a lack of accessibility; from Root & Kerr, infra note 13 at 15.
[13] From C. Kenopic, Keeping Hands in Motion (Canadian Association of the Deaf, 2000) citing J. Root & D. Kerr, The Employment and Employability of Deaf Canadians (Canadian Association of the Deaf, 1998) at 6.
[14] Root & Kerr, ibid. at 36.
[15] Ontario Building Code Act, S.O. 1992, c. 23.
[16] Ontario Human Rights Commission, Policy and Guidelines on Disability and the Duty to Accommodate (March 2001) available online at www.ohrc.on.ca.
[17] Citizenship and Immigration Canada, Senior Immigrants (65+) Landing in Ontario in 1999, by Official Language Ability, found in Aging Quiz, Third Age Ontario Intranet Web site, supra note 5.
[18] Statistics Canada, Mother Tongue of Aboriginal Seniors, Ontario, 1996, online: Third Age Ontario Intranet Web site, supra note 5.
Employment
Employment is fundamental to ensuring equal participation and equal opportunity in society. It has a direct bearing on a person’s economic status while the person is in the workforce and afterwards. Therefore, any examination of age discrimination in employment must consider the effects of practices and policies on the person while they are working as well as after they have retired. It must also consider the effect on society as a whole.
Employment is not just related to economic considerations. For many people, employment is fundamental to their sense of dignity and self-worth. It promotes independence, security, self-esteem and a sense of participating in the community. Discriminatory treatment and involuntary termination of employment therefore have an effect that is more than financial.
Most individuals and organizations that participated in the consultation were concerned with age discrimination in employment. Many people reported having been affected by employment related age discrimination, either themselves or through a family member or friend. They described the hardship and sense of loss that accompanied being excluded from the workplace due to age. Others expressed a sense of moral outrage at the fact that persons can be forced to retire at age 65 and that those who do continue to work after 65 lose human rights protections against age discrimination.
Mandatory Retirement and the Lack of Protection for Workers over 65
...there are significant public policy reasons to re-examine mandatory retirement at this time to determine whether the arguments based on social utility should continue to justify what is otherwise a discriminatory practice.
Mandatory retirement is age discrimination. Making a decision solely on the basis of age, and not on the basis of a person’s ability to perform the essential duties of the job, is a form of unequal treatment. As a society, we would not find it acceptable to terminate someone’s employment in such a fashion if the reason were related to another ground in the Code such as race, sex or disability. Therefore, there are significant public policy reasons to re-examine mandatory retirement at this time to determine whether the arguments based on social utility should continue to justify what is otherwise a discriminatory practice.
Background
No law in Ontario requires persons to retire at any age. In theory, employees can work until they no longer wish to do so or are incapable of performing their jobs. However, many workplaces have retirement policies that require all employees to retire at age 65. These may arise out of collective agreements negotiated between the employer and union or as a result of an employer’s personnel policies. For the reasons discussed below, employees who do not wish to retire at 65 have no means to challenge the collective agreement or personnel policy. This means that in effect, an employer can impose mandatory retirement at 65.
The Ontario Human Rights Code defines “age” as:
s. 10(1) “age” means an age that is eighteen years or more, except in subsection 5(1) where “age” means an age that is eighteen years or more and less than sixty-five years.
The restricted definition of age means that the Commission cannot receive a complaint of age discrimination in employment from someone who is 65 or older. This means it is not contrary to the Code for employers to require employees to retire at age 65 (or older) and employees cannot challenge this practice. Similarly, workers who continue to be employed cannot complain if their employer treats them differently (e.g. in remuneration, benefits, hours, vacation etc.) on the basis of their age.
Restricted definitions of age, or other exceptions in human rights legislation that permit mandatory retirement at age 65, have been the subject of several challenges under the Canadian Charter of Rights and Freedoms. In all of the cases, the Supreme Court of Canada has upheld mandatory retirement. In one case, the Supreme Court considered the definition of "age" in the Ontario Code and found that, mandatory retirement policies do discriminate on the basis of age but are a reasonable limit on the equality rights of older persons (McKinney v. University of Guelph (1990)[19]).
Since court challenges have been unsuccessful, in order for mandatory retirement to be made illegal, it is necessary to amend the Code. Only the Legislative Assembly of Ontario can amend the Code. In a 1977 Report, Life Together: A Report on Human Rights in Ontario,[20] the Commission recommended that the definition of age be amended to remove the upper limit so that the ability to perform the job would be the only criterion for determining when a person should leave employment. That suggestion was not acted upon by the Legislature at that time.
The Impact of Mandatory Retirement
Many individuals and organizations told the Commission that imposing retirement has a significant financial impact. People expressed a fear that they would lose their homes, face a significant drop in their standard of living or even find themselves in a state of poverty. Consultees noted that they are responsible for supporting others, such as family members with a disability or university-aged children, and that they will not be able to do so if they are no longer permitted to work. They are very worried about the consequences of their retirement on their loved ones.
Mandatory retirement can have a particularly serious financial impact on some persons. Women have traditionally played a caregiver role and stayed at home to raise or care for family members. At the same time, women who are part of the paid labour force tend to work in sectors where employer pension plans are not available, are more likely to work in part-time or temporary employment and earn considerably less then men. Women are therefore doubly disadvantaged: they have no income and no Canada Pension Plan (CPP) contributions for the years they do not work and for the years that they do work, they are unlikely to be able to build up CPP, RRSP or private pension plan credit to retire to a decent standard of living. They are, therefore, at real risk of being forced into poverty as a result of mandatory retirement (see section on Age & Gender for statistics on low income and gender). Moreover, women who took time off for family responsibilities may have to retire just as they reach the peak of their careers.
One woman described returning to employment in her 50s, after having raised a family, as a result of marital breakdown. Her employer did not have a mandatory retirement policy, however, one was instituted as she was approaching age 65. She retired on a very inadequate pension and her request to keep working in a situation that would enable her to still contribute to the pension was denied. However, after retirement, she returned to work with the same employer on a contract basis . She is no longer entitled to contribute to her pension, is no longer eligible for paid vacation and has no job security.
Recent immigrants face the same difficulties as they may have a shorter period of employment in Canada upon which to build a pension. They, along with visible minorities and Aboriginal persons, also tend to have restricted access to the labour market and lower incomes.[21] Similarly, persons with disabilities also tend to experience greater unemployment and lower wages during their working lives.
There are other reasons why persons may experience hardship if forced to retire. People are starting their families later in life, or are starting a second family, and may have dependant children when they reach the age of 65. Rising education costs mean that it is not unusual for parents to assist their children through college and university. Many employees need to maintain their earning power through this time and beyond to ensure an adequate standard of living for themselves upon retirement.
The financial impact of mandatory retirement has been described as follows:
“This year [our son] completed university and has been accepted and started post graduate studies in Pharmacy. Because I will be forced to retire June 22, 2002 my son will be forced to take on extra debt and I will have to dip into my savings to help him for his final two years.” (Alfred J. Herman)
“...I will only have 24 years credit in their pension plan, hardly enough to retire on. Presently I have one daughter just finished university, another daughter in university and a son beginning community college, therefore at this time saving for retirement is extremely difficult.” (James G. Watson)
“If I should not be able to find gainful employment in the future solely on the criteria of my being over 65 years old, I will lose the capability of keeping my home.” (Don Pelz)
Being told that one is no longer a valued employee, solely because of one’s age, has a profound psychological and emotional impact. Indeed, many commented that they had either themselves experienced, or observed in others, a real loss of interest in life’s activities after being forced to retire.
“The singular most important element in human mental health is their work or what they do. A strong argument can be made that forcing retirement on people is directly affecting their health, an issue that is right at the core of human rights.” (Ken Shields)
The impact on human dignity is best illustrated using the words of consultees:
“Did you ever feel like an old pair of worn out shoes? Well that can happen. You feel rejected and no longer of any value in the workplace or your community.” (Mervyn Morley)
“My new subsidized income, along with my feeling of professional uselessness has shown me one thing, the reality of how society views and treats the aging.” (Grace Watson)
“The psychological trauma that is associated with forced retirement could be easily avoided if we are given a choice.” (Michael Nippalow)
Many people noted that treating someone who was a good employee at age 64 as incompetent the day they turn 65 is irrational: “To arbitrarily declare that at age 64 you are capable of work and at age 65 you are no longer capable of work is ridiculous and discriminatory” (Raymond Carter).
Re-examining Mandatory Retirement
To demonstrate the arbitrariness of age 65, one participant described the story of how it was selected:
“Count Bismark was asked to provide a pension for retired government clerks and asked...by what age are most of them dead? He was told 65 and he said, fine, 65 will do.” (Prof. Irwin Pressman)
In addition to the negative impact of mandatory retirement on individuals, and other human rights based considerations, there are several compelling reasons to re-examine mandatory retirement at this time. In fact, we must seriously reconsider the wisdom of forcing the retirement of people who wish to continue working.
Aging population: As the baby-boom generation ages, in the next few years there will be a significant number of persons approaching age 65. Moreover, due to longer life expectancies, people are living significantly past age 65 (on average about 20 years past 65). This means that the utility of requiring people to retire at 65, an age designated at a time when it was rare to live that long, must be questioned. In 30 years, almost one quarter of Canada’s population will be 65 and older (Prof. C.T. Gillin & Prof. Thomas R. Klassen). Having fewer workers support retired persons over a longer period of time will likely have significant ramifications for our economy.
Economic considerations: The Commission was repeatedly told that common sense dictates that it is better for society to reap the benefits and contributions, in particular tax revenues, of having people working rather than drawing income from the state.
Labour shortages: Labour shortages are currently being experienced in certain sectors, such as health, education and construction, and this is predicted to increase when the baby-boom generation retires. For example, the Commission was told that in the context of university professors: “[We] can’t find qualified people...there is a huge shortage of qualified people available, and at the moment we are forcing them to retire here.” (Faculty Group, Carleton University). A recent newspaper article reports that retirees are being enticed back to work to address shortages of skilled labour.[22]
A related concern can be described as ‘brain drain’. The Commission was told that highly skilled and qualified older workers are moving to the United States so that they will not be subject to mandatory retirement. The result is a significant loss to workplaces, hospitals, universities and society as a whole (Faculty Group, Carleton University). Ontario must examine policies, such as mandatory retirement, that are causing talented, experienced people to relocate.
Trends in the United States and Internationally: Other countries, most notably the United States, New Zealand and Australia have eliminated mandatory retirement without major consequences. The Commission was told that the greater productivity and the lower unemployment rate in the United States has been attributed to more flexible labour market regulation (Prof. C.T. Gillin & Prof. Thomas R. Klassen). The experience of other countries demonstrates that eliminating mandatory retirement in Ontario should not prove as problematic as some would argue.
The United Nations has said that state parties to the International Covenant on Economic, Social and Cultural Rights, should expedite the trend towards the elimination of mandatory retirement.[23] The Group of Eight leaders have noted the need to foster the economic participation of older persons.[24] Given that Canada is a State party to the Covenant and a member of the Group of Eight, Canada should take a leadership role in acting upon these recommendations.
Promoting Fairness: In addition to the unfairness inherent in being excluded from the labour force on the basis of age, consultees noted other issues of fairness. Some employers allow workers to stay on past 65 while others do not. Therefore, two people performing essentially the same job can find themselves in completely different circumstances. In some cases, employees are hired back to do an identical job but without many of the benefits of full-time, regular employment. Moreover, many commented that for the majority of their tenure with an organization, there had been no mandatory retirement. They found it unfair that their employer, and in some cases their union, could impose such a significant change to the terms and conditions of employment as they approached age 65.
Many individuals and organizations noted the irony that some of the most powerful, respected and influential persons in Canada, including the Prime Minister and other politicians, judges and senators, are not subject to mandatory retirement at age 65. Many of these people are over the age of 65 and are valued for their years of experience. Numerous people commented that this sort of ‘double standard’ is not acceptable.
Justifications for Mandatory Retirement
It is necessary to examine common justifications for mandatory retirement to see if they are sufficiently compelling to offset human rights concerns.
To facilitate planning: An argument has been made that mandatory retirement is necessary to allow employers to plan for their staffing needs. However, it does not appear to the Commission that this rationale has relevance in today’s highly dynamic workplace. Mandatory retirement at 65 arose when workers tended to work full-time for the same employer for many years. Now employees are highly mobile. Leaves of absence related to pregnancy, illness and professional development are commonplace. Moreover, even with mandatory retirement, many workers choose to retire before age 65 and the timing of early retirement varies from person to person. As one author has noted:
...uncertainty is inherent in the running of most organizations. In the area of human resources specifically, turnover, absenteeism, disability and death are all uncertain, probabilistic flows that organizations have to cope with. General approaches, processes and techniques that are used by organizations to forecast these flows can be adapted to forecast the delayed retirements that may occur under flexible retirement policies.[25]
Therefore, it does not appear that this rationale is sufficiently sound to justify mandatory retirement.
To promote job opportunities for youth: This argument is largely based on impression rather than evidence. In other words, people simply assume that mandatory retirement will facilitate the hiring and promotion of younger workers. However, this assumption may not reflect reality. One author notes that no study can be cited to demonstrate that the termination of older workers through mandatory retirement directly caused the hiring of younger ones.[26]
In workplaces and jurisdictions that do not have mandatory retirement, very few workers choose to stay past age 65 and those who do tend to retire within a year or two. Moreover, this argument relies on the “lump-of-labour” fallacy: that there are a fixed number of jobs that must be allocated among workers so that “every job held by an older worker is one less job available for a younger one”. The workforce does not function in this fashion and older workers are rarely retiring from jobs that younger workers are seeking. Moreover, opportunities for younger workers exist without having to retire older workers. In many fields there are shortages of workers and employers are unable to find employees to fill positions. This will be discussed further in the next section.
In addition, as many people have noted, arguing that discrimination against one group is acceptable as it promotes opportunities for another group is offensive to human rights principles. Society has not accepted this argument in other contexts, for example the claim that any job occupied by a woman is one less job for a man. Given that age discrimination can have the same financial, psychological and emotional impact as any other type of discrimination, it should not be used to justify this form of discrimination.
To ensure that workers leave with dignity: Employer representatives told the Commission that mandatory retirement allows older workers to leave the workforce with dignity. If mandatory retirement is abolished employers will be obliged to manage performance and even terminate older workers who are having difficulty performing job duties. The argument is that this is a hardship both for the employer and the employee. It is said that mandatory retirement allows individuals who are under-performing to leave the workforce in a socially acceptable fashion with a level of income security. The Commission was told that employers would prefer to be able to offer the option to work past 65 where there is a need and an employee can perform the job.
The Commission also heard that mandatory retirement should not be a substitute for appropriate personnel policies such as progressive performance management. While it may mean more work for employers, performance issues of workers who are nearing age 65 should be handled in the same way they would for any other employee. Treating older workers the same way as co-workers and evaluating them on the basis of actual performance, rather than age-based assumptions, best promotes their dignity. Given the small number of workers who chose to work beyond 65, it likely that employers will rarely be forced to take performance-related steps to terminate the employment relationship.
Employees should have an equal opportunity to remain in the workforce. However, the current legal environment allows employers to re-hire selected employees under conditions that are less favourable than the pre-retirement situation. This has the potential to create a ‘second-class’ group of employees. Indeed it is of significant concern to the Commission that workers who do remain employed after age 65 cannot make a complaint of age discrimination if subjected to unequal terms and conditions of employment.
To control costs: A concern has been expressed that abolishing mandatory retirement will result in significant costs to employers with respect to long-term disability, group life insurance and pension contributions. It is also argued that if employers cannot rely on mandatory retirement and must terminate employees who cannot perform their duties, they will have associated costs, for example severance pay and the cost of defending wrongful dismissal suits. It was noted that since a number of programs and systems rely on age 65 as the retirement age, a sweeping review of laws and policies will be needed.
The Commission agrees that these issues would require further consideration and that a revision of several statutes and programs may be necessary. Nevertheless, this should not represent an obstacle to reconsidering mandatory retirement. To the extent that increased costs to the employer may be an issue, it can be addressed. For example, the Code and the Employment Standards Act already allow some distinctions to be made on the basis of age in pension and group insurance plans.
Options for Dealing with Mandatory Retirement
The Commission was told that employees want choice and that retirement should not be seen as an ‘all-or-nothing’ proposition. Rather, flexible or phased-in retirement should be the goal. This could involve part-time work, job sharing, moving to a different job, such as a consultant or trainer, or being assigned new responsibilities.
Employers will not be required to retain employees who are unable to perform the essential duties of the job. However, those who wish to continue working should be permitted to do so, regardless of their age, if they can perform their jobs. Employers should adopt performance management programs and apply progressive performance management to all employees regardless of age. Employers who wish to have a blanket retirement policy, at any age, will be required to demonstrate that the policy is based on bona fide occupational requirements (e.g. as is the case with current policies that require firefighters to retire at age 60).
Some have suggested that there should be no upper limit on how long a person can work and that the ability to perform the job should be the only consideration. Others have suggested moving the retirement age from 65 to 67, 70 or 75. However, in the Commission’s view, a blanket mandatory retirement defence set at any age can raise identical human rights and public policy concerns as compulsory retirement at age 65. As individuals live longer and healthier lives and demonstrate an extremely variable range of physical and mental abilities, it appears that age-based retirement benchmarks will be difficult to justify.
Abolishing mandatory retirement should not result in people being penalized if they choose to retire before age 65. It is not intended that a review of mandatory retirement will result in an expectation that people should continue to work longer. Rather, it is merely intended to allow those who want to continue to work to have that choice.
Lack of Protection for Workers Over 65
The Commission is very concerned that persons who are not subject to mandatory retirement and who continue to work past age 65 cannot bring a complaint of age discrimination in employment. Given that more people may find themselves in this situation, particularly in light of demographic trends and labour shortages, this has the potential to affect an increasing number of people. It the Commission’s view that it could not have been the intention of the Legislature to exclude this category of workers from human rights protections and that steps should be taken to address this anomalous situation.
Recommendations for Government & Community Action
13. THAT the Code be amended to eliminate the blanket defence to mandatory retirement at age 65 and to extend protection against age discrimination to workers over 65. This could be done by removing the upper limit of 65 in the definition of “age” in section 10(1). Employers who wish to have age-based retirement policies will be required to demonstrate that the policy is based on bona fide occupational requirements. Laws and programs that require consequential adjustment should also be reviewed.
14. THAT, irrespective of whether the Code is amended, employers and unions reconsider the utility and necessity of requiring employees to retire at age 65 and revise their retirement policies and collective agreements to promote flexibility and choice.
Workplace Age Discrimination
The input received on workplace age discrimination served to confirm the problems identified in the Commission’s Discussion Paper. In particular, many reported that stereotypes and negative attitudes towards older workers (starting as early as age 45) are commonplace in the workplace. This includes assumptions that older workers are less ambitious and hardworking, less dynamic and unable to learn new things. People reported being denied training opportunities and opportunities for advancement and being terminated because of age. Others recounted the difficulties they had in finding employment due to their age. The Commission heard about job-seekers colouring their hair and removing years of experience from their résumés in order to appear younger.
Many people agreed that older workers bear the brunt of workplace reorganization and downsizing. Others commented that being asked whether a person would like to retire might be interpreted as “being pushed to make the decision” (The Canadian Association of the Deaf).
During the consultation process, the Commission heard that older workers would like to be given the same opportunities as everyone else to demonstrate their skills and abilities and to be treated as valued members of the organization without ageist stereotypes or assumptions being applied. They would like to be hired, trained and promoted at the same rates as their younger counterparts.
Several of the individuals and organizations consulted stressed the need for the Commission to educate the public and employers about ‘myths and realities’ with respect to older workers. This is necessary to assist employers but also to ensure that co-workers do not treat older employees with disrespect. The following are examples of common myths and realities[27]:
Myth: Job productivity declines with age.
Reality: Some productivity decrease is observed with some types of work but not others. In some work settings, studies show older workers are more productive than younger ones. Overall, chronological age accounts for minimal differences in job performance.
Myth: Older workers decline in physical capacity.
Reality: While there is some decline in physical capacity, a supportive work environment can overcome the effects of this change and age is not necessarily a limiting factor in physically demanding work even through the 60s.
Reality: There is some slowing down with age in reaction time and speed of performance, but older workers do as well or better than younger workers on creativity, flexibility, information processing, accident rates, absenteeism and turnover.
Myth: Older workers can’t learn new things.
Reality: With appropriate training methods and environments, they can generally learn as well as younger workers.
Other suggestions included encouraging employers to be ‘45+ friendly’ and acknowledging those who are supporting older workers. The benefits of employing older workers should be stressed. For example, older workers may be settled in a community and may stay longer in a job, they may have fewer family commitments because children have grown and they may be more receptive to part-time work or job sharing (Halton Region’s Elderly Services Advisory Committee (ESAC)).
With respect to investigating human rights complaints, several tools were suggested to distinguish between age discrimination and legitimate decisions based on non-discriminatory reasons: evaluating the ratio of 45+ employees to total employees, looking at the number of employees who have held employment in the company for over 15, 20, 25 or 30 years, reviewing the number of 45+ employees who have been hired and tracking the resumes received from 45+ candidates to see if they are receiving equal consideration (Diana Ward, Award Personnel).
Several consultees noted that employees themselves need further information about what constitutes age discrimination and their rights and recourses if they find themselves in such a situation: “Older workers may not be cognizant of the fact that they are being discriminated against in relation to their age. The may actually lack awareness of ageism issues” (Wendy Draper).
The Commission is grateful for these suggestions and will consider them further as it develops its public policy statement on age discrimination.
Recommendations for Government & Community Action
15. THAT employers take steps to ensure that workplace policies and procedures do not have an adverse effect on older workers. Workplace human rights policies and education programs should address age discrimination and harassment.
16. THAT workplaces should be free of ageist assumptions and stereotypes and employers should ensure that older workers are afforded the same opportunities as their younger counterparts. The value of older workers should be recognized.
Commission Commitments
3. The Commission will engage in public awareness activities to educate employers and employees about their rights and responsibilities under the Code, to dispel the myths that are often associated with older workers and to encourage employers to view older workers positively.
[19] [1990] 3 S.C.R. 229.
[20] Ontario Human Rights Commission, Life Together: A Report on Human Rights in Ontario (Toronto: Ontario Human Rights Commission, July 1977).
[21] See Canadian Race Relations Foundation, Unequal Access: A Canadian Profile of Racial Differences in Education, Employment and Income (Report prepared for Canadian Race Relations Foundation by the Canadian Council on Social Development, 2000).
[22] A. Lawlor, “Retired but in demand” St. Catharines Standard (30 April 2001).
[23] In particular, General Comment No. 6: The Economic, Social and Cultural Rights of Older Persons, United Nations Committee on Economic, Social and Cultural Rights, E/C.12/1995/16/Rev.1.
[24] From the Kyushu-Okinawa Summit Meeting, 2000, G8 Communiqué, 23 July 2000 cited in submission by Prof. D. Gorham, Faculty Group, Carleton University.
[25] N.C. Agarwal, Mandatory Retirement and the Canadian Human Rights Act (Prepared for the Canadian Human Rights Act Review Panel, October 1999) at 19. Reproduced with the permission of the author.
[26] Ibid at 21.
[27] Agarwal, supra note 25 and submission provided by Diana Ward, Award Personnel.
Housing
“Government does not recognize housing as a human right.”
(Older Women’s Network)
Throughout the consultation process, the Commission heard concerns about the need for more accessible and affordable housing and for special needs housing for seniors including those who are homeless. Submissions also highlighted that the principle of “aging in place” is central to any discussion, policy or program efforts concerning housing for older persons.
Affordable Housing
Inadequate housing options: Almost every submission that discussed the issue of housing emphasized the critical need for more affordable housing for older persons. The Ministry of Municipal Affairs and Housing (MMAH) told the Commission that it has implemented several programs to address the issue of affordable housing. MMAH has expanded the Rent Supplement Program, a program that provides housing subsidies to individuals living in privately owned rental housing. Additionally, the government has committed $50 million annually to assist low-income individuals and families, including seniors, across Ontario. MMAH also introduced tax credits to encourage the construction of new affordable multi-residential rental accommodation.
“There are many older people among the homeless... the lack of accessible low cost housing and the removal of rent controls have left many seniors fearful of eviction. There is no place to go.”
(Canadian Pensioners Concerned)
Despite these expansions and investments, the Commission heard that the current approach to affordable housing for older persons is inadequate. The fact that the Canada Mortgage and Housing Corporation(CMHC), and MMAH are no longer guaranteeing new mortgages, in combination with the transfer of responsibility for housing to the municipalities, means that there is little new affordable housing available. This, in addition to the fact that increases in pension income have not been consistent with the increases in rental costs, creates a particularly vulnerable state for older persons. As one group noted, some of the current housing options that exist for older persons are only available to those who can afford to pay (Dieticians of Canada). To address this gap, more affordable housing, priced at fixed rents, or larger increases in pension income are necessary (ESAC).
The Tenant Protection Act, 1997: The Commission heard a great deal about the impact of the Tenant Protection Act, 1997[28] (the TPA) upon older persons. MMAH told the Commission that the TPA provides a number of protections, particularly for frail older persons and those living in care facilities. As well, MMAH emphasized that the TPA prohibits discrimination in accommodation (rental housing) on the basis of age, among other grounds.
“A lot of tenants don’t consider it a tenant protection act; they don’t see themselves as protected.”
(Senior Link)
Despite this, the Commission heard from organizations and individuals alike that the TPA has served to remove a number of real protections for older persons. The removal of rent controls was identified as having an impact on the availability of affordable housing, a particular problem for women and older persons on fixed incomes. The result is that older persons may not have sufficient income to choose where they wish to live. For example, the Commission heard about widowed women facing barriers in obtaining smaller, more manageable residences because of the ability of landlords to raise the rent for new leases.
The Commission was also told that the TPA is of particular concern for older persons who are at risk of homelessness. As Senior Link suggested, older persons are likely one of the fastest growing groups of homeless persons because they are socially and economically vulnerable. The Older Women’s Network added that this is particularly so for older women who experience disproportionate social and economic disadvantage. The TPA increases this vulnerability by making it easier for landlords to evict people.
Homelessness: For those who are homeless, the issue of affordability is even more critical. Without income and a permanent address, homeless older persons face great barriers in the search for stable housing. Consultees told the Commission that in a housing market with little or no affordable housing, the vulnerability of this group of older persons is heightened.
Options for Addressing Affordability
“Subsidized housing has the potential to reduce the likelihood that an older person will live in dire poverty... be in need of a food bank or possibly become homeless and not have enough to eat.”
(Ontario Coalition of Senior Citizens’ Organizations)
To address the issue of affordability, a number of the submissions suggested that the provincial government take steps to ensure that affordable housing is widely available. New and creative housing initiatives are required including housing options developed through partnerships with for-profit and not-for-profit agencies. Subsidies for low-income seniors in rental apartments should be considered. Consultees suggested rent subsidies through the Guaranteed Annual Income Supplement (GAINS) for low-income seniors who rent in apartments, nursing homes and retirement homes (Canada’s Association for the fifty-plus (CARP)).
Additionally, submissions suggested that care facilities should include a variety of rental options by including some units at market rent, and some at subsidized rates.
Finally, the need for shelter allowances similar to programs such as the Section 8 Voucher program in the United States or the Shelter Allowances for Elderly Renters (S.A.F.E.R.) program in Manitoba was identified (Fair Rental Policy Organization of Ontario (FRPO)). Additional suggestions included the restoration of rent controls and incentives and grants to municipalities for subsidized housing for older persons.
Social housing
Social housing in Ontario consists of three types of housing: non-profit, public and co-operative housing. Such housing is meant to provide affordable accommodation for those who face barriers in the rental accommodation market based on income, age, social and health related needs. [29] MMAH submitted that the new Social Housing Reform Act, 2000 provides a mechanism by which the provincial government will implement standards to protect the supply of housing for people with special needs, including the frail elderly. The new Act also includes provisions directing municipal service deliverers to maintain the number of units for people with special needs, and to provide mandatory priority access to all social housing units designated for people with special needs.
Despite such legislation, consultees expressed great concern regarding access to appropriate social housing. The Commission heard that a person in need of social housing in Toronto must currently wait seven years (The Ontario Coalition of Senior Citizens' Organizations). Additionally, one group noted that within the existing stock of social housing, buildings cannot be made accessible in a safe and cost effective manner. Therefore, construction of new special needs housing should be the focus (FRPO).
The Older Women’s Network recommended that the provincial government again become involved in building and maintaining affordable social housing. They noted that in the absence of incentives for builders to develop social housing, the only way for it to become available will be through investment by various levels of government.
Accessible housing
“A barrier-free environment should not simply be the “aim” but rather the expected standard for all buildings.”
(ARCH)
Throughout the consultation process, the Commission heard that the current stock of housing (including care facilities) for older persons is not accessible to several groups of older persons. Consultees emphasized that housing for older persons, whether a private home or a residence, must be equipped and accessible so that residents are afforded a life of dignity, independence, full-participation, fairness and security.
Barrier-free Design: The Commission heard that in the design of housing for older persons, fire exits, entrances and general living spaces should be free of barriers, and ramps should be available for those who cannot use stairs. Accessibility also means that hallways and doorways should be wider to accommodate the need for walkers or wheel chairs, counter tops should be lowered for future possible use by residents in wheelchairs, and bathrooms should have grab bars and be wheelchair accessible (United Senior Citizens of Ontario). Still others suggested that flooring should not be slippery; windows should be lowered and bright lighting should be used; door knobs and other fixtures should be selected bearing in mind the needs of persons with arthritis; and living quarters should have enough storage for wheelchairs, walkers and oxygen tanks. Inclusive design that takes into account the specific and evolving needs of older persons as they age is critical.
“Developers and builders must design housing that is ‘senior friendly’ and consider the needs of the disabled. This expertise is now available. If necessary, make changes to the Ontario Building Code.”
(Alliance of Seniors to Protect Canada’s Social Programs)
The Commission learned about the barriers faced by Deaf, deafened, the hard of hearing and visually impaired older persons as a result of the current standards for building design. As the Canadian Hearing Society noted, many buildings that house Deaf, deafened or hard of hearing older persons are not equipped with appropriate supports, resulting in the potential for safety risks, for example in the case of emergencies. In order to meet the needs of Deaf, deafened, and hard of hearing persons, buildings should include: flooring with enough give to allow for audible foot-stamping to attract attention, and clear visual signage and indicators such as flashing alarms, phones and doorbells, TTYs and caption decoders. Additionally, there should be extra insulation between suites as older persons who are hard of hearing may have to turn up the volume on their televisions or radios. Finally, the Commission heard that the building design needs of persons with visual impairments include open spaces, round corners, clear and gentle lighting, restful wallpaper and paint, and Braille signage.
Consultees emphasized the need for education with respect to barrier-free design and flex-housing as important priorities for those involved in the design and construction of homes for older persons. Additionally, it was suggested that the provincial government provide grants to municipalities for the construction of barrier-free subsidized housing and financial incentives for builders to encourage them to meet the housing needs of older persons (CARP and ESAC). With specific reference to the Deaf community, the Canadian Association of the Deaf emphasized that all levels of government must work in partnership with the Deaf community to devise strategies that ensure nursing, retirement homes and other housing options are accessible to Deaf older persons.
Housing options for older persons should recognize the desire for contact with the community and should serve to encourage independence and full-participation in the process.
Access to the Community: The Commission heard that in addition to physical accessibility, housing for older persons must also encourage access to the community. Housing and care facilities for older persons should be close to amenities such as stores and transportation and near to other people. As one group noted, older women “really want to be close to the community so that they can go to church, they can go to the post office, they can go do a bit of shopping, they can go themselves to the drug store...as long as they are mobile, this is their wish” (Older Women’s Network). Housing options for older persons should be developed with the concept of community in mind and encourage the interaction of older persons and younger persons (United Generations Ontario).
Flexible housing: Housing options for older persons should also be designed to adapt to the changing needs of people throughout the aging process. Options should be available based on a continuum of care so that older persons are not required to continually move as physical and/or mental abilities decline (Dieticians of Canada). The Commission heard that the ideal housing option for older persons is linked housing developments that would include supportive housing, nursing homes, subsidized seniors-only housing and some market rent options in addition to amenities such as health clinics, and recreational and educational programs (United Senior Citizens of Ontario). Several groups emphasized such housing options should be available in rural and urban areas so that, regardless of where an older person resides, the option of remaining within one’s own community exists.
Aging in Place
“It is important that every person have the right to live wherever they want to live and [decisions regarding] living arrangements [should ] not just be based on the fact that they have a hearing loss or that they’ve gotten older.”
(The Canadian Hearing Society)
Many of the groups emphasized that "aging in place" is critical to the promotion of independent living for older persons. The Commission heard that most older persons want to remain in their own home and the concept of aging in place is key to fulfilling this desire. As the Canadian Hearing Society and the Ontario Association of Non-Profit Homes and Services for Seniors noted, it is important that every person have the right to live wherever they want to live and that decisions regarding living arrangements should not be based solely on aging or the experience of a disability. The Canadian Mental Health Association told the Commission that academic research promotes “aging in place” as a critical element in the health of older persons and as an economical housing strategy responsive to the needs of taxpayers. As such, this concept must be central to any strategy for developing housing options for older persons.
In order for “aging in place” to be realized for older persons, affordable and accessible housing options and in-home supports must be available (Chatham-Kent CCAC). One individual noted that older persons might have little or no choice as to where they will live if they do not have the financial means or family support to remain in their own community. Several groups noted that currently, the availability of in-home supports is limited or not available at all. As Over 55 (London) Inc. told the Commission, community-based services that can allow older persons to “age in place,” including services such as housekeeping, home maintenance, and the provision of nutritious meals, must be supported.
Consultees suggested garden suites (independent housing established on the property of family members) as a housing option that could allow older persons to remain within their own community. Municipal regulations govern the construction of garden suites and stipulate that such units can exist only on the property of a relative. One group suggested that these rules should be amended to allow older persons to occupy garden suites on properties owned by persons other than relatives. This type of arrangement would allow non-relatives to provide support when relatives are not present or do not exist (ESAC). In addition, a number of groups suggested “granny flats” and basement apartments in the homes of family members. However, some cautioned that in some cases, these living arrangements can foster abuse and isolation rather than independence, dignity and full-participation.
Recommendations for Government & Community Action
17. THAT municipal, provincial and federal governments should cooperate to develop a strategy for affordable housing for older persons in Ontario. Options for consideration include rent subsidies, shelter allowances and rental cost protections for older persons. The concept of “aging in place” should be a central consideration.
18. THAT all levels of government engage in efforts to ensure that the social housing supply in Ontario meets the existing and future needs of older persons and other vulnerable groups.
19. THAT the Ontario Building Code Act, 1992 be amended to incorporate the best principles of barrier-free design.
20. THAT developers and builders design and implement barrier-free housing that responds to the specific needs of older persons, including those with disabilities.
Commission Commitments
1. The Commission will develop a discussion paper on housing and human rights that will address issues facing older persons.
[28] Tenant Protection Act, 1997, S.O. 1997, c. 24.
[29] Social Planning Unit, Community Services Department, Regional Municipality of Niagara, Social Housing Niagara - Social Housing Newsletter, Vol.1, Issue 1, October 1999, at 1.
Health care, institutions & services
“Basic health care is a foundation in our society and differences are never justifiable. Seniors’ needs are real and they surely deserve easy access to basic health care in the same manner afforded to other groups in Ontario.”
(Chatham-Kent CCAC)
The submissions received by the Commission consistently mentioned the barriers faced by older persons in the areas of health care, institutions and services. The Commission heard about concerns with the current health care system, including: insufficient funding and the resulting inadequacy of community-based care, the shortage of care professionals; and a number of concerns regarding long-term care facilities. Submissions mentioned physical barriers such as building accessibility and social barriers such as restrictive attitudes within the health care system as major obstacles facing older persons. Similarly, the Commission heard that physical and social barriers exist in the area of general services, and a number of consultees noted barriers specific to transportation. The message offered by participants throughout the consultation process was clear: barriers to health care, institutions and services serve to adversely affect the dignity, self-worth, independence and full-participation of older persons in the province of Ontario.
Community-based care: limited funding and services
Insufficient funding of community-based care was identified as a critical barrier for older persons seeking access to the health care system. The Ministry of Health and Long-term Care (MOHLTC) told the Commission that “significant investments have been directed to the expansion of long-term care community services designed to help people remain in their own homes for as long as possible.” The Commission was pleased to learn that MOHLTC committed to an investment of $1.6 billion in long-term care community services for the fiscal year 2000-01, of which, $1.1 billion is for Community Care Access Centres (CCACs). Another $448 million of that investment is for other long-term care community services such as adult day programs and attendant care services.
“The Ministry recognizes the long-term care service system as an essential component of an integrated health service system and is committed to ensuring a quality system of community and facility long-term care services.”
(Ministry of Health and Long-Term Care)
Despite such investments, the Commission heard about concerns regarding the insufficient funding of community-based services resulting in diminished capacity to appropriately address the health care needs of older persons. The Chatham-Kent CCAC indicated that over 50% of the population that they serve are older persons. However, the chronic under-funding of CCACs serves to severely limit their capacity to address the unique care needs of older persons. They noted that due to an emphasis on cost containment, they have been forced to reduce their caseload from 3,000 to 2,600 persons daily, translating into approximately 200 fewer older persons receiving care daily. Without appropriate funding, CCACs told the Commission that it is difficult to respond to the current demand for services.
“Many seniors cannot access physicians because there is such a shortage of physicians and because seniors with health problems require an above average amount of time and attention... available physicians do not welcome seniors as patients.”
(CCAC Timiskaming)
Health care for older persons is unique and requires an approach that takes into account evolving needs throughout the process of aging. A number of groups told the Commission that the care needs of older persons often demand more time of care professionals. However, the health care system in Ontario is not funded to allow care providers to spend the appropriate amount of time tending to their unique health care needs. The Advocacy Centre for the Elderly emphasized this very point in stating, “ there are maximum limits with respect to services...strict limitations on the amount of hours [of care] you can get...in no way [do they] meet the needs of many seniors in the community... that’s what we are finding with many of the services...It is the system itself, the structure that has the negative impact on the older person because the hours aren’t there, the time isn’t there to deal with the senior.”
Addressing this very issue, the Chatham-Kent CCAC noted that due to inadequate funding, they have been forced to reduce the hours of home support from 12 to 16 hours per week down to currently less than eight hours per week. The Ottawa-Carleton CCAC added that the Long-Term Care Act, 1994,[30] sets limits on the quantity of services that CCACs can provide to older person within the community. They noted that as a result, the level of community care can, at times, be insufficient to address the health care needs of older persons. In the context of early discharge and a shortage of convalescent care beds, they stated that older persons are often discharged into the community without a comprehensive care plan. For those older persons in need of longer periods of convalescent care, this can translate into lives at risk.
“If we want to keep people in the community and out of hospitals, you need to find the money to do so. When we have a shortage of beds and therefore discharge people after a very short period of time, they go home very frail and are still very much in need of help at home...they suffer like everybody else from a lack of medical care services, but more so because they are so vulnerable.”
(Ontario Association of Social Workers)
A number of submissions also emphasized that the inadequate funding of community-based services negates that capacity for older persons to “age in place”. As the Ottawa- Carleton CCAC noted, in order for older persons to be able to remain within their own communities, there is a need for an expansion of the care currently provided by CCACs and government-sponsored residential care facilities. In the context of inadequate funding, several groups noted that this is difficult to achieve.
The Older Women’s Network and the Ontario Association of Social Workers emphasized that the Commission should not forget those older persons who are most marginalized within the context of the current system of community-based care. Older women who have disabilities, are poor, are from diverse racial and/or ethno-cultural backgrounds, or are lesbian or transgendered suffer “double jeopardy” in the context of community-based care. Age discrimination, in addition to exclusion based on other personal characteristics, means that vital community-based services are even more difficult to access.
In response to these concerns, a number of the consultees recommended that funding must be made available so that CCACs and others providing care to older persons have the capability, both in terms of resources and time, to provide the highest level of care. Multidisciplinary services, including community-based care, rehabilitation, chronic and complex continuing care and supports such as nursing care, home support services, therapies and case management services, should receive the appropriate focus in funding. The Ontario Association of Social Workers recommended that Commission policy initiatives related to age, “must encourage and promote equal access to a comprehensive range of community-based services and supports regardless of age or other attributes”.
“We know that elderly people and their families want assurance that care in a long-term care facility will be available when care in the home and community is no longer possible. The expansion and redevelopment facilities (nursing homes and charitable homes for the aged) are specific goals of this Ministry.”
(MOHLTC)
Long-Term Care Facilities: Barriers and Concerns
MOHLTC told the Commission that it recognizes the importance of long-term care as a key element of Ontario’s health system, and has committed to investment in long-term community-based and facility services. It told the Commission that, “in 1998, to meet the needs of a growing elderly population, Government announced support for the construction of 20,000 new long-term care facility beds and the redevelopment of approximately 16,000 existing beds. This investment in long-term care beds is $602.4 million”. Recognizing that residents of long-term facilities have increasingly complex needs, MOHLTC also introduced new design standards and guidelines for long-term care facility design in 1998. These standards and guidelines will apply to the 20,000 new beds and 16,000 renovated beds expected to be completed in 2004.
Furthermore, MMAH told the Commission that through the protections provided under the TPA, it maintains its role in the regulation of care homes. MMAH said that protections include the ability of care home tenants to terminate their tenancies with 30 days notice; the requirement that care providers give tenants written tenancy agreements outlining care and meal services to be provided; and the requirement that care providers provide tenants with information packages regarding the cost and availability of meal and care services and emergency services.
Nevertheless, a number of the submissions identified concerns with long-term care facilities in Ontario. The Canadian Mental Health Association highlighted the shortage of long-term care beds. They told the Commission that, at times, this has resulted in the inappropriate placement of older adults who experience mental health issues, a particularly vulnerable group of older persons.
Senior Link and a number of other groups highlighted the concern regarding the lack of regulation of rest and retirement homes. The Commission was told that the lack of regulation in such facilities allows for substandard care to exist and the abuse of older persons to occur (Ontario Coalition of Senior Citizens’ Organization and Canadian Pensioners Concerned). ARCH (A Legal Resource Centre for Persons with Disabilities) expressed concern about “the indiscriminate use of physical restraints in institutions on elderly patients and the psychologically disabled”. Another group noted, “low income seniors are at a disadvantage because they have to take what they can afford in a retirement home which may be sub-standard (Alliance of Seniors to Protection Canada’s Social Programs)”. A number of groups told the Commission of the need for monitoring, standards and legislation that will ensure appropriate care and safety for older persons living in retirement residences. The need for a Residents’ Bill of Rights was highlighted. CARP specifically recommended that the provincial government take responsibility for developing the necessary legislation and standards.
Alternatively, the Chatham-Kent CCAC suggested that MOHLTC should enhance the capacity of the Ontario Residential Care Association (ORCA) to enable it to self-regulate the industry. The MOHLTC submission provided insight into government action on this issue. It noted that “with funding assistance from the government, the Ontario Residential Care Association (ORCA) is expanding its self-regulatory program for retirement homes [to include] a consumer complaint investigation system and the development of a checklist for consumers on what to look for in a resident’s contract with a retirement home.” Details as to the progress of this expansion were not provided.
Several groups expressed concern regarding the cultural, linguistic and religious needs of older persons living in long-term care facilities. One group noted that not all ethnic groups have their needs addressed equally within such facilities. Dieticians of Canada noted that the cultural, linguistic and religious needs of older persons must be given equal consideration. They suggested that the provincial government support the development of educational packages to be used in long-term care facilities that would assist staff in providing appropriate and respectful care (for example in the provision of food, religious observation and culturally specific social activities).
The Canadian Association of the Deaf and the Canadian Hearing Society expressed great concern regarding the treatment of Deaf older persons in long-term care facilities and senior residences. The lack of TTY systems, visual alarms in bedrooms, hallways and bathrooms, and shake awake alarms means that Deaf persons are placed at risk and excluded within their own living spaces. There is a critical need for more residences specifically designed for Deaf seniors given that there currently exists only one (The Bob Rumball Centre for the Deaf) in the entire province. Several groups noted that this issue is further compounded for those living in rural areas where programs for Deaf persons may not be available at all. It was recommended that all levels of government, in partnership with the Deaf community, must work to ensure that nursing homes and retirement homes are accessible to Deaf older persons (Canadian Association of the Deaf).
“Current practices tend to generalize and treat all people over the age of 65 as identical...this can unfairly limit access to required services for people with Alzheimer Disease, ultimately threatening the independence and dignity of this growing segment of the population.”
(The Alzheimer Society of Ontario)
The Alzheimer Society of Ontario raised specific concerns regarding the treatment of persons living with Alzheimer Disease while residing in long-term care facilities. MOHLTC told the Commission that, “half of the residents in facilities have Alzheimer Disease or related dementia.” The Alzheimer Society of Ontario emphasized that this group has unique needs, however, “current practices tend to generalize and treat all people over the age of 65 as identical...this can unfairly limit access to required services for people with Alzheimer Disease, ultimately threatening the independence and dignity of this growing segment of the population.” As well, the way in which funding levels for long-term care facilities are determined, does not take into account the cognitive and behavioural care needs of persons with Alzheimer Disease. This impacts on the ability of care facilities to appropriately address the needs of this growing group of older persons.
Others expressed concern regarding the independence of certain groups of older persons in care facilities. The Canadian Mental Health Association noted that sometimes, a conflict of rights occurs, wherein the right of an older person to live at risk comes into conflict with the rights of caregivers to intervene. The Ottawa-Carleton CCAC stated that staff in institutions must be knowledgeable of the older person’s right to refuse treatment or care, a right that must be respected, even if it leaves the older person at risk. The Ontario Association of Social Workers emphasized that health decision-makers within long-term care facilities must take seriously and support the wishes and decisions of the older person in care. With respect to end of life decisions, the Alzheimer Society of Ontario added that, “it is the right of all individuals to be able to make choices regarding end of life and to have those choices respected. In Ontario, legislation exists to protect this right, however, the legislation is not always followed, for example, when family members are vigorously opposed to an Advance Directive or the decision of the Substitute Decision Maker.”
Finally, a number of organizations commented on the barriers faced by older couples once they reside in a care facility. Dieticians of Canada noted that older couples face difficulty in obtaining accommodation in the same room, the result of which can be “forced separation” of the couple. Anxiety and loneliness can occur as a result. This, in turn, can have a negative impact on the older couple’s health and well-being. Separation may also occur due to differing levels of care required by the couple. They suggested that multi-level care facilities that can address varying levels of care would assist in ensuring older couples are not forced to live separately. As noted earlier, ACT and CLGRO added that gay and lesbian couples face considerable barriers in care facilities, given that at the outset, their relationships are often not even recognized or validated.
The focus on acute care
“Health care for seniors takes second place to other aspects of the health care system. Comparative spending on community health care and long-term care, whose target population is primarily seniors, is a fraction of the health care spending for acute care.”
(Chatham-Kent CCAC)
A number of the submissions noted an emphasis on acute care, which diverts attention from the long-term care needs of older persons. Senior Link told the Commission that, “in the process of hospital restructuring, what we have found is that community-based care has become acute care...long-term care has been put on the shelf...” The Alzheimer Society of Ontario emphasized that the focus on acute care means that, “elderly people, particularly those with chronic diseases like Alzheimer Disease or related dementia are not able to get adequate services, or in some cases any services at all.”
A shortage of knowledgeable health care professionals
Consultees also noted that access to health care professionals who are knowledgeable about the aging process is a key concern, particularly in the context of the growing population of older persons in Ontario. The Alzheimer Society told the Commission that its own research has revealed that minimal amounts of teaching time are currently allocated to the issues of aging and dementia in Ontario medical schools. As they and others noted, “[the] lack of training in these areas will lead to barriers for older adults who need to utilize the health care system and will compromise the quality of care and/or access to appropriate care” (Alzheimer Society of Ontario).
The Commission also heard that it is very difficult for older persons without a physician to obtain one (KFL&A CCAC). The CCAC of Timiskaming told the panel that accessibility to health care is limited by the shortage of physicians throughout Ontario. To address this issue, they suggested “incentives for physicians to specialize in geriatrics”. It was emphasized that because many physicians no longer make home visits, accessibility is limited for some older persons. The Commission heard that this issue is compounded in rural communities where the access to doctors, and in particular specialists, is “virtually non-existent”. As the number of older persons increases, these problems will intensify. The Canadian Mental Health Association – Windsor-Essex, branch added that as a result of shortages in physicians, nursing staff and personal support staff, inadequate and inappropriate care can result.
To address the shortage of physicians within the province, MOHLTC told the Commission that it has implemented the “Underserviced Area Program” to attract and retain health care providers within the northern, rural and remote areas of the province. The program includes “financial incentives for physicians willing to relocate to under serviced areas, recruitment initiatives, practice supports and enhancements to access to medical services for affected communities”.
Barriers to health care information
The Commission heard that a number of groups of older persons are not receiving information about health care services, thereby limiting access. They emphasized that while CCACs have services to offer, many older persons are either unaware of the existence of CCACs and the availability of their services or are reluctant to ask about them. Additionally, the Commission was told that internet-based communication is not very effective in reaching older persons. Consultees noted the need for outreach so that older persons throughout Ontario are aware of the services that are available. CCACs indicated that with additional funding, they would acquire greater capacity to do so.
The Commission learned about barriers to health information that extend beyond the issue of public education. Issues such as language and citizenship status pose particular barriers for certain groups of older persons:
“We have often found that a family will be reunited in Canada and [the older person] will not have citizenship status and that leaves them very vulnerable because they cannot access the health care system.”
(Senior Link)
The Ontario Association of Social Workers noted health care and other service providers must ensure that linguistically appropriate services are available: “services in the language of the elderly person is of course crucial...[service providers should] make it a policy to employ people who speak the language of the people [they] are serving”. In addition, they noted that CCACs should ensure that their materials are published in various languages.
“Health care, long-term care, elder care, mental health service providers, employed by the public and private sectors must be provided with in-service training to give them a better understanding of ...the use of various communication strategies for Deaf, deafened and hard of hearing people.”
(The Canadian Hearing Society)
The Canadian Hearing Society noted that Deaf, deafened and hard of hearing older persons experience communication barriers in the context of health care services. It told the Commission that staff within the health care system are unable to communicate with older persons who experience hearing loss. The Supreme Court of Canada’s decision in Eldridge v. British Columbia (Attorney General),[31] has confirmed that sign language interpretation, where necessary to ensure equal access to health care, must be provided. Nevertheless, consultees indicated that while the decision was a significant milestone, its implementation has been slow.
It is the Commission’s view that health care providers in Ontario should abide by the Eldridge decision by providing sign language interpretation to respond to the needs of Deaf persons. As consultees noted, it would appear that health care and other service providers should be trained in appropriate communication techniques that respond to the needs of Deaf, deafened and hard of hearing people.
Cost as a barrier to access
The consultation revealed that a critical barrier for older persons is the limited access to health care benefits often experienced in later life. Many employer drug benefit programs cease on retirement or termination. Those who are too young to be eligible for the Ontario Drug Benefit plan, or those who find themselves “in-between” private coverage are often required to pay for health related products and services. Some older persons may not be able to afford to do so.
Canadian Pensioners Concerned emphasized the reality of cost as a barrier to health care services for older persons. They told the Commission that the costs of prescriptions can sometimes place older persons in a position of choosing between buying medicine or other necessities of life. This can, in turn, lead to a life at risk. The Alzheimer Society of Ontario added that drugs to treat Alzheimer Disease cost approximately $5 per day, creating a significant barrier for older persons who are not covered by a health plan or the Ontario Drug Benefit (ODB). As they noted, “without coverage, many adults do not have access to timely interventions that can maximize quality of life and minimize their stress, anxiety and caregiver burden.” Dieticians of Canada added that, “coverage of nutrition supplements [under the ODB] is not adequate. Many of Ontario’s elderly, whether living at home, in retirement homes or in long-term care facilities are experiencing complications of malnutrition.” The Commission was told that to address this issue, MOHLTC should work to expand the types of prescription drugs and alternative therapies that will be covered for older persons by the Ontario Health Insurance Plan (OHIP).
“More and more seniors are having to resort to the use of food banks because they can’t afford to buy food and the very expensive drugs which are often prescribed but not included on the list covered by the provincial health plan (The Ontario Drug Benefit)...the alternative is to go without drugs.”
(Canadian Pensioners Concerned)
Older persons who have or may develop a disability also experience barriers because of the cost and availability of assistive devices. The cost related to assistive devices presents a significant barrier, particularly since those who may need them most may be the least likely to be able to afford them.
Even where government funded assistive devices programs exist, they may only offset some of the costs or pay for basic technology instead of better devices that would improve an individual’s quality of life. In addition, age limits in the provision of such programs pose another barrier and have been challenged as a form of age discrimination. For example, in Ontario (Human Rights Commission) v. Ontario (Ministry of Health)[32] the Court of Appeal found that the Ontario Ministry of Health’s Assistive Devices Program could not restrict the provision of closed circuit television magnifiers only to persons under the age of 25. A 71-year-old man had been refused this visual aid. Additionally, the Commission has recently initiated a complaint against the MOHLTC and its contractor, the West Park Healthcare Centre, for using age-based criteria in the provision of assistive devices. Under the program, access to incontinence devices is restricted to persons born after July 1, 1963, thereby excluding older persons.
Consultees also mentioned the cost associated with dental benefits as a significant barrier for older persons. The CCAC of Halton noted that “Ontario does not have a universal dental program for seniors [and]...the majority of older adults are without dental insurance”. It told the Commission that without a dental plan and with limited income, older persons do not access regular dental care. This can result in poor oral health leading to “physical, psychological and social problems”. Dieticians of Canada and the CCAC of Halton noted the importance of good oral care to the ability of an older persons to maintain weight and avoid “systemic health problems”. The need for affordable and accessible dental coverage for older persons was emphasized as a critical aspect of any efforts to address the health-related needs of older persons in Ontario (Halton Health Department).
Social barriers to access
Throughout the consultation, the Commission heard about the social barriers to accessing health care and institutions experienced by older persons. The Ontario Association of Social Workers told the Commission that, “older adults are frequently characterized as non-contributing members of our communities and their need for services [are] portrayed as being a drain on scarce public resources”. The Ontario Coalition of Senior Citizens’ Organizations and others told the Commission that older persons are often labelled as “bed-blockers”. The Ontario Association of Social Workers added that this labelling of older persons, “infers that patients who are legitimately in need of long-term care beds are partially responsible for the shortage of emergency room beds...[and] shifts attention away from the vitally needed public debate about government priorities and funding for our health care system”.
“The health care system tends to place priority on those who are younger and those who are working...If you are older, the younger person gets to the top...that is age discrimination.”
(Canadian Pensioners Concerned)
A number of organizations told the Commission about the impact of ageist assumptions upon the care of older persons. Canadian Pensioners Concerned told the Commission that older persons in Ontario are the last to be considered when it comes to health care services. The Canadian Mental Health Association provided the Commission with an example of how this is experienced by older persons. It told the Commission that older persons, particularly those facing mental health issues, are often faced with the comment “what do you expect for your age” when they meet with health care professionals. A number of groups added that some physicians “normalize” concerns of older persons, often relating them to the aging process and, in turn, providing inadequate assessment and follow-up.
The Ontario Coalition of Senior Citizens’ Organizations emphasized that older persons are often identified as a lower priority for surgical procedures and are often over-prescribed medication. Additionally, a couple of organizations expressed concern that powers under the Canada Health Act could allow for health care providers to limit access to health care procedures on the basis of age. A number of the consultees, including the Chatham-Kent CCAC noted that they had heard anecdotal evidence of doctors limiting the access of older persons to procedures and to their practice. As ESAC told the Commission, the health care system in Ontario must provide older persons with the same level of care and consideration as would be provided to a younger person.
The Canadian Mental Health Association, Windsor-Essex branch, told the Commission that for older persons experiencing mental health issues, ageist assumptions continue to compound their marginalization within the health care system. Such attitudes lead to insufficient levels of attention paid to the mental health needs of older persons. They told the Commission that this frequently results in the use of chemical or physical restraints that have been documented in research as leading to further deterioration. The Ontario Coalition of Senior Citizens’ Organizations noted that older persons also experience infantalization at the hands of health care providers and that when an older person requires admittance to a hospital, they are often faced with resistance, particularly if the person is also experiencing mental health issues. Karen Henderson emphasized that in response to such treatment, “there is a critical need for training to be instituted for health care providers so that they may be equipped to address the health care needs of older persons in a manner that is effective and respectful of human dignity”.
“There is a critical need for training to be instituted for health care providers so that they may be equipped to address the health care needs of older persons in a manner that is effective and respectful of human dignity.”
(Karen Henderson)
General Services
“The Canadian Hearing Society would recommend that you, the Human Rights Commission, urge the Secretary of Cabinet and the Deputy Minister of Management Board Secretariat to ensure that all Ontario Ministries are aware that the Ontario Human Rights Code requires their services, including contracted services, be accessible to all older people with disabilities.”
(The Canadian Hearing Society)
A number of consultees said that ageism and age discrimination extend beyond health care services into other areas of service delivery. The Canadian Centre for Activity and Aging told the Commission that older persons are “politely discriminated against” by virtue of the fact that many public buildings and facilities are not accessible. As the Golden Years Club of Lakefield pointed out, access to buildings for older persons, particularly those who experience a disability, remains an issue of access to services. They told the Commission that municipalities should ensure that municipally owned buildings are accessible. Canadian Pensioners Concerned and others noted that there is a strong need for a disability act and a [revised] building code in Ontario that would require service providers to ensure that their buildings and services are fully accessible. The Advocacy Centre for the Elderly noted that, “ the impact of this type of legislation, if made mandatory compliance and if applied to all sectors (not just government), could result in a great improvement in services and systems for seniors”.
Several organizations told the Commission that older persons who are Deaf, deafened and hard of hearing face additional barriers to services because of the systemic exclusion that they experience throughout their lives. The Canadian Association of the Deaf told the Commission that the major barriers tend to be systemic and economic discrimination. The Canadian Hearing Society told the Commission that the shortage of persons trained and available for interpretation presents a substantial barrier for older Deaf persons. The Canadian Association of the Deaf added that barriers are created when a hearing person refuses to pay for interpretation services or when funding is unavailable to cover the costs related to interpretation and other forms of accommodation. As well, they noted that older persons may face communication issues when younger interpreters do not recognize or understand the signs used by older persons. This can lead to frustration and a loss of confidence as to whether others are receiving their information correctly. The Commission heard that when appropriate supports, such as interpreters, are available and accessible for Deaf seniors’ a greater balance of power is had and self-determination encouraged because they are able to express their needs and concerns in their first language.
Others reported that older persons also face attitudinal barriers in the area of services. The Advocacy Centre for the Elderly told the Commission that they receive complaints regarding the paternalism experienced by older persons at the hands of service providers. It noted that older persons are often labelled as “hard-to-serve” clients. At other times, they are treated as if they are incapable and when important decisions are required, service providers often defer to family rather than to the older person him or herself. It explained to the Commission that, “in the end it has a discriminatory effect upon the older person because they are not involved in the service delivery themselves... it exacerbates the situation and lessens the contact they have with the service provider”. Clearly such practices negate the principles of dignity, independence and full–participation for older persons in such circumstances.
“The paternalism we see in service delivery...we receive complaints from seniors who identify that they are not the people being dealt with in terms of services...its their family...[seniors] are not treated as the decision maker or they are treated as if they are incapable.”
(Advocacy Centre for the Elderly)
Transportation Services
Many of the submissions identified the same concerns that the Commission noted in its recent Discussion Paper on Accessible Transportation Services in Ontario. Senior Link told that Commission that, “the transit system and wheel trans are not accessible for many seniors who need assistance getting to a doctor or into a hospital...they need to be supported so that seniors can access programs...in rural Ontario, this issue is amplified because of the isolation and the lack of transit”. Canadian Pensioners Concerned echoed this concern and told the Commission that for older persons, particularly those with mobility impairments, transportation is extremely limited and this can lead to isolation from family, community and from the general activities of daily living. One group told the Commission that, “ travel to the doctor, dentist, or store for rural seniors is very difficult...if they cannot drive or there is no public transportation, they must rely on family or home support” (Council on Aging for Renfrew County). Given what the Commission heard about limitations in community-based supports and the availability of physicians, transit inaccessibility compounds the barriers to health care and other services for older adults.
“The populations of many small communities have a large proportion of seniors. These communities do not now have, nor have [they] ever had, public transportation. This restricts seniors from accessing health, social and commercial services in larger centres. Recognize that any policy initiatives will have a different effect in the rural north than in, for example, Toronto, Ottawa or Sudbury.”
(CCAC Timiskaming)
A number of organizations strongly emphasized the need for more accessible transportation. Ramps, elevators, escalators and low floor and lift-equipped buses are critical for ensuring equal participation of older persons with disabilities. Bright lighting, contrasting floor materials and audio announcements make it easier for persons with low vision to use public transit. TTY phones and written announcements improve accessibility for persons who are Deaf, deafened or hard of hearing. As the Canadian Hearing Society (London) noted, public transportation buildings often are not equipped with sufficient and proper TTY equipment or public address systems. Others noted that in addition to physical barriers, older persons often face “poor treatment” by public transportation employees signalling the need for sensitivity and awareness training to address such social barriers (The Ontario Coalition of Senior Citizens’ Organizations).
For those who cannot access even a well-integrated conventional system, there is a need for parallel para-transit services. The Commission heard, however, that the eligibility criteria for many para-transit services may disentitle older persons with certain types of disabilities, e.g., disabilities that arise from respiratory problems, heart conditions, and cognitive impairments resulting from stroke, dementia or brain tumours, and sensory disabilities. Consultees also noted that even those who are eligible find that para-transit services are not adequate to allow them equal access to public transit.
The Commission heard that while there have been some improvements over the last few years, transportation in Ontario remains inadequately funded. The Ontario Coalition of Senior Citizens’ Organizations noted that evidence of under-funding can be found in the area of volunteer escort services provided by MOHLTC. It told the Commission that such services are only available for medical appointments. Transportation that would allow older persons to attend social and recreational activities is either unavailable or limited. ESAC recommended the implementation of creative solutions to the transportation issues facing older persons in urban and rural areas. They suggested a subsidized taxi program while Senior Link recommended community-based volunteer networks based in local organizations that could provide older persons with transportation to their various appointments. Dieticians of Canada suggested that, “Municipalities, District Health Councils and the Ministry of Health and Long-Term Care need to support the development of funded transit systems and review eligibility so that transit is available to all who need it”. The Older Women’s Network simply suggested that to address the transportation issues facing older persons, all levels of government should provide subsidies and invest appropriate amounts of money to ensure that an adequate system of transportation is available.
Recommendations For Government & Community Action
21. THAT medical schools and training centres for health care professionals and others who work with older persons enhance education on the needs of older persons.
22. THAT health care institutions, facilities and services be made accessible to all older persons, particularly those with disabilities.
23. THAT the government should exercise caution in the use of age-based criteria in health care programs such as assistive devices, prescription drug and dental programs.
24. Consistent with the Eldridge decision, that service providers provide sign language interpretation services where necessary to ensure equal access for persons who are Deaf, deafened and hard of hearing.
25. THAT the provincial government take further steps to regulate rest and retirement homes. Issues to address might include a Resident’s Bill of Rights and standards for the use of restraints and end-of-life decisions.
Commission Commitments
5. The Commission will communicate with the Ontario College of Physicians and Surgeons, the Ontario Medical Association and the Canadian Medical Association and other appropriate organizations to advise that unequal access to medical treatment and other health care services on the basis of age or disability may constitute discrimination.
6. The Commission will contact and meet with professional faculties such as medicine, nursing, dentistry, nutritional sciences and social work to discuss the urgent need to include comprehensive education on age discrimination within their curricula and to ascertain their plans for including such education in their programs.
7. The Commission will continue to take steps to promote accessibility amongst service providers throughout Ontario.
[30] Long-Term Care Act, 1994, S.O. 1994, c. 24.
[31] Eldridge v. British Columbia (Attorney General), [1997] 3 S.C.R. 624 at para. 96.
[32] (1989), 10 C.H.R.R. D/6353 (Ont. Bd. Inq.), aff’d 14 C.H.R.R. D/1 (Ont. Div. Ct.), rev’d 21 C.H.R.R. D/259 (C.A.).
Elder abuse & neglect
“Elder abuse and neglect should be identified as abuses of human rights.”
(Canada’s Association for the Fifty-Plus (CARP))
Many individuals and organizations provided comment on the issue of elder abuse. The submissions emphasized that elder abuse is a human rights issue requiring an effective response by government and by communities throughout Ontario. The Commission heard that any action concerning elder abuse, whether by government, community organizations or by individual caregivers, must be grounded in a respect for the dignity, independence, full participation and the security of older persons. The following pages provide an overview of the comments offered to the Commission throughout the consultation process.
Although a universal definition of the term elder abuse does not exist, Health Canada has defined it as “the physical, psychosocial or financial mistreatment of a senior”. [33]
Physical abuse of an older person can include assault, rough physical treatment, sexual exploitation, or the failure to provide an older person with food, or with appropriate personal, hygienic or medical care. Psychosocial abuse includes verbal abuse, the social isolation, the failure to provide affection, and the denial of the opportunity to make or take part in decisions concerning one’s own life. Financial abuse includes the mishandling of an older persons money or property, and also includes fraud. [34] However, a 1999 report by the Ontario Legislative Assembly adds to this list a number of additional forms of elder abuse including: medication abuse (e.g., the misuse or withholding of medications), the denial of fundamental rights and freedoms, abandonment, and self-neglect.[35]
Financial abuse tends to be most common (62.5%), with verbal and physical abuse second most common (35% and 12.5% respectively) followed by neglect (10%).[36] Submissions received by the Commission highlighted that elder abuse and neglect occur in all contexts; in the home, in hospitals, in long-term care facilities, and in retirement homes.
The Under-Reported Nature of Elder Abuse
The Commission heard that approximately 4% or 60,000 of the 1.5 million older persons living in Ontario experience elder abuse.[37] However, many older persons are not willing to report elder abuse because of the social stigma attached to it or because of concern regarding the consequences of reporting a loved one or caregiver. As a result, this percentage may be under-estimated.[38]
A number of the submissions highlighted the complex nature of elder abuse. As one group told the Commission, the dependency of older persons upon their caregivers means that abuse inflicted by a caregiver is more difficult to address. The embarrassment experienced by older persons who are abused by their family members and caregivers makes elder abuse a “hidden form of familial abuse” (The Ontario Association of Social Workers). Older persons who are experiencing abuse are often faced with the decision of whether or not to report their abuser, the result of which could mean the loss of their caregiver, making their decision to report that much more difficult (Chatham-Kent CCAC). Others told the Commission panel about the serious dilemma facing older persons who are abused by those for whom they themselves are caring for, wherein the older person’s desire to care for that person conflicts with their own need for safety.
CARP discussed the issue of elder abuse in the context of care facilities. It noted that for those who experience abuse within care facilities, fear can act as a real deterrent to reporting abuse. A number of consultess told the Commission that families may also be too afraid to complain about the abuse of their older relatives because they fear retribution against their loved ones in the form of poorer care or further abuse (ARCH and Karen Henderson). As the Council on Aging noted, the problem of elder abuse is very much like domestic violence and requires a systemic approach to ensure that victims of elder abuse are not further victimized in the process of seeking recourse and in defending their rights.
Abuse of Deaf and “Deaf-Plus” Older Persons
Several consultees told the Commission of the particular experience of elder abuse faced by Deaf, deafened and hard of hearing older persons. While Deaf seniors experience the same forms of abuse as other seniors (e.g., financial abuse, physical abuse, emotional abuse, etc.), they also experience communication abuse. The communication barriers faced by Deaf older persons makes this group particularly vulnerable to the other various forms of abuse (The Canadian Association of the Deaf). The Canadian Hearing Society provided the Commission with several anecdotal descriptions of situations of communication abuse:
“A client who went into hospital uses hearing aids and speechreads. The client needed information from the nurse regarding her medical situation. The nurse refused to turn on the light so the client could speechread, even though the client requested it and told [the nurse] why.”
“[A] Client’s medical condition [was] discussed over the person’s head to a third party rather than being discussed with the client.”
“A colleague of mine had a client who was misdiagnosed with dementia and was hospitalized. It took my colleague a year to get that person out of the psychiatric ward and back home...he had been tested without his hearing aids in.”
The vulnerability that occurs in the context of elder abuse is heightened for “Deaf-Plus” older persons, that is, those who experience hearing impairment in addition to other disabilities such as blindness, Cerebral Palsy or intellectual disabilities. This group of older persons is often the easiest to abuse because they are vulnerable and unlikely to report the occurrence of abuse (The Canadian Association of the Deaf). The Canadian Association of the Deaf emphasized that, “people with this kind of special vulnerability often simply do not know where to go or how to seek assistance, so they endure the abuse as being almost a birthright of ‘superior’ hearing people”.[39]
A report by the Canadian Association of the Deaf entitled, Keeping the Hands in Motion[40] highlighted the communication barriers faced by “Deaf-Plus” older persons. For those who have arthritis in their fingers or hands, the ability to communicate through sign language and writing is limited. Given the importance of vision for Deaf persons in communication, where a person experiences a visual impairment, communication barriers are further compounded. These barriers further exacerbate an older person’s vulnerability in the context of an abusive situation.
Throughout the consultations, organizations emphasized the need for broad public education and awareness building with respect to elder abuse and neglect. Others suggested the need for targeted education, particularly geared toward professionals who work with older persons on a regular basis (i.e., doctors, nurses, social workers, etc.). In addition, a number of consultees called for more education and supports for caregivers.
With respect to Deaf and Deaf-Plus older persons, the Canadian Association of the Deaf suggested that a network of advocates should be set-up to assist Deaf seniors with abuse and neglect-related issues, to protect Deaf seniors from abuse and ensure that they are aware of their rights. Others suggested that more funding should be provided to develop educational programs that could alert Deaf and Deaf-Plus older persons to the issues of elder abuse, neglect issues, to their rights and to possible mechanisms of recourse.
Causes of and Contributors to Elder Abuse
“Until the elderly are fully recognized as individuals with the same human rights...as other citizens, abuse of the elderly will prevail – whether it takes place in the home, community or institutions.”
(Ontario Association of Social Workers)
The Commission heard that the causes and contributors to elder abuse are varied and extensive. A number of submissions noted that ageism and a general negative attitude toward seniors is a key underlying contributor to elder abuse. ESAC told the Commission that elder abuse is tied to a lack of services in the community as well as the lack of available long-term care beds and available, affordable and accessible housing. Still others noted that the economic and social vulnerability of older persons contributes to elder abuse.
The Ontario Coalition of Senior Citizens’ Organizations told the Commission that elder abuse frequently occurs when primary caregivers experience “burn-out or significant stress”. This includes professional caregivers who are facing a growing caseload, as well as complex care responsibilities within the context of an under-funded system of services. This also refers to family caregivers who are expected to provide care for aging relatives in the context of dwindling government services and supports. Reports by Health Canada and the Government of Nova Scotia also support this notion. They both report that elder abuse can result when a caregiver’s stress is exacerbated by a lack of available information and resources about caring for an aging person. Furthermore, a caregiver’s own issues such as unemployment, substance abuse, personal relationship problems and unresolved family conflict can contribute to the occurrence of elder abuse.[41]
Submissions noted that many well-intentioned adult children or other caregivers want to make decisions for older persons, especially when they perceive that an older adult cannot make decisions for themselves. However, a number of organizations noted that seniors often lose their rights to self-determination, independence and dignity in the process (Ontario Association of Social Workers and The Canadian Mental Health Association). As Health Canada’s work on elder abuse notes, the denial of the opportunity for an older person to make or take part in decisions concerning his or her own life can be a form of psychosocial abuse. The Canadian Mental Health Association suggested that in order to ensure that an aging person’s rights to independence and dignity remain in tact, widespread public education is needed.
The lack of regulation of privately-run care facilities was also noted as a contributor to the vulnerability of older persons to abuse. The need for regulation of privately-run care facilities and for standards for all such homes across the province was discussed in the section on Health Care, Institutions & Services.
The lack of emergency shelters available for older persons who have experienced abuse was also mentioned as a factor that contributed to elder abuse. The Ottawa-Carleton CCAC told the Commission that existing emergency shelters are often full and tend to address the needs of younger women and children. Such facilities are not appropriate for older persons and options for people suffering abuse by caregivers are limited. Other organizations told the Commission that barriers to accessing shelters include a general lack of knowledge on the part of older persons regarding how to access emergency shelters. Furthermore, language and cultural barriers exist that further limit the accessibility of these facilities. ESAC suggested that temporary shelters should be established to aid older persons and those with disabilities in their transition from an abusive situation to a safe environment. The Ottawa-Carleton CCAC suggested that shelters should exist for both men and women, should be walker and wheelchair accessible and staffed with people who are able to address the complex needs of older persons.
Programs to Combat Elder Abuse
A number of organizations told the Commission about programs to combat abuse of older persons. One such program is Phone Busters, a program implemented by the Ontario Provincial Police. Phone Busters accepts calls from across North America from older persons who have fallen victim to telemarketing fraud. Representatives from Phone Busters told the Commission that, “80 per cent of the people that call Phone Busters are seniors [and] have lost money to telemarketing fraud”. Others added that single older women are particularly vulnerable to financial “scams” such as telemarketing fraud. As with other forms of abuse, financial abuse of older persons is under-reported. Phone Busters estimates that, “only one per cent of the losses are actually being reported due to embarrassment and shame on the part of the victim”.
“We are teaching them to [regain] their dignity because a lot of [older persons] are embarrassed and will not talk to their family members...If you lost [money], the last thing you would want to do is tell your children...”
(Ontario Provincial Police, Phone Busters)
The statistics for the Phone Busters program illustrate that it has been very successful in reducing the dollars lost by older persons who are vulnerable to financial abuse. As a result, the group sought new mechanisms through which further outreach to older persons could occur. The result was a partnership between the Near North CCAC and Phone Busters to implement an elder abuse hotline pilot study. The pilot is aimed at addressing systemic abuse, neglect, physical and psychological abuse of older persons. The Commission was told that the six-month pilot ended early this year and that the Ministry of Citizenship, Seniors’ Secretariat will determine the next steps for the program.
Recommendations for Government & Community Action
26. THAT mechanisms currently in place to address other forms of familial abuse should be extended to apply to elder abuse.
27. THAT the provincial and municipal governments take steps to support specialized programs, including shelters, for victims of elder abuse.
Commission Commitments
8. The Commission will continue to monitor the outcomes of the provincial plan of the Round Table for Ontario’s Elder Abuse Strategy that are within its mandate.
[33] Health Canada, National Clearinghouse on Family Violence, Elder Abuse, at 1, online: Health Canada ,<http://www.hc-sc.gc.ca/hppb/familyviolence/html/eldereng.html>.
[34] Ibid.
[35] Andrew McNaught for the Ontario Legislative Library, Legislative Research Service, Elder Abuse Prevention Laws (Office of the Legislative Assembly of Ontario: Toronto, 1999) at 2.
[36] Ibid at 2.
[37] This is supported by the August 1999 study by the Ontario Legislative Library, supra note 35 at 2.
[38] The Ministry of Citizenship, Seniors’ Secretariat notes that up to 10% of the 1.5 million seniors in Ontario experience elder abuse. See “Putting a Stop to Elder Abuse” online document at <www.gov.on.ca/mczcr/seniors/english/elder-abuse-update.htm>.
[39] Ibid at 27.
[40] Kenopic, supra note 13 at 10.
[41] Government of Nova Scotia, Ministry of Community Services, Fact Sheet 7: Elder Abuse, online document at <www.gov.ns.ca/coms/facts7.htm>.
Elder care
The Commission heard that elder care is a growing need, and largely provided in the community by family members. As well, the gendered nature of elder care and the disproportionate burden that women face in caring for aging relatives was noted. Consultees described the stress caused by caring for older persons and the need for efforts to address caregiver stress. Finally, the Commission heard that issues relating to elder care require creative responses by government in terms of legislation, programming and funding and by employers in terms of workplace flexibility to ensure that caregivers are supported in their provision of care. The message presented to the Commission was that caregivers are fulfilling an important societal role and should not have to bear the responsibility alone. Society should be supportive of their efforts.
“Informal caregivers are...silent victims in a silent system...they have inherited unfair burden and responsibility without enough support in the downloading of responsibility [as a result of] hospital closures.”
(Canada’s Association for the Fifty-Plus (CARP))
The Squeeze in Elder Care
A number of organizations told the Commission that that there is mounting pressure in the area of elder care: as the population continues to age, hospitals continue to discharge patients at a faster rate and inadequate provincial funding is provided to community based health care providers. These factors together make it difficult for home care providers to provide adequate care (The Council on Aging). This means that families will increasingly be required to provide care for their aging relatives. Submissions by the Council on Aging and others highlighted that in this context, older persons themselves will become the victims of an inadequate system, particularly those older persons who do not have family or the capacity to access private health care.
The Gendered Nature of Elder Care
A report submitted by CARP noted that in 1999, 46% of all working Canadians provided general eldercare.[42] The Older Women’s Network told the Commission that the care of older persons is most often performed by women; 90% of paid caregivers are women and a significant proportion of informal caregivers are also women. This is supported by a recent report by the Ontario Community Support Association.[43] Canadian Pensioners Concerned told the Commission that the role of women as primary caregivers has existed as a “norm” within society, requiring women to place caregiving responsibilities above their own aspirations. They noted, “because of family responsibilities, lower salaries, and fewer opportunities for education and job promotions, [women] have been unable to amass sufficient retirement income through pensions and savings”. The gendered nature of elder care therefore has repercussions for women in other areas, likely to last far into their later lives.
Caregiver Stress
Caregiver stress has been identified as a significant and increasingly important issue as the number of older persons requiring care in the community grows. One individual told the Commission that caregiving places a significant burden upon families, particularly when family members do not have the necessary training to provide appropriate care for their aging relative. The Chatham-Kent CCAC noted that particular expertise is required in the care of older persons given that elder care often requires knowledge of polypharmacy and diseases related to aging, and the know-how to deal with consent and capacity issues. Without such expertise, stress can be further compounded. A number of submissions emphasized that the burden experienced by the family can also cause stress for the older person because it can cause the older person to feel like a burden. The Ottawa-Carleton CCAC and others stated that for older people who are caring for another older person, this burden can be exacerbated by their own care needs.
Accommodating Caregiving
The Consultation Paper asked for comments on the extent of an employer’s duty to accommodate employees who care for older persons. A number of organizations responded with creative suggestions that could apply in the workplace and beyond. ESAC told the Commission that support for caregiving in the form of job flexibility is necessary. They stated that the ten days of emergency leave to care for family members, as prescribed by Subsection 50(5) of the Employment Standards Act, 2000[44], is not enough in most cases. ESAC suggested that leave to care for family members should be flexible, similar to the current provisions for maternity leave. The Ottawa-Carleton CCAC suggested that temporary leaves and reassignments are possible options to help employees address caregiving obligations. The Alzheimer Society of Ontario added that, “there is a need for employers to offer provisions such as a leave of absence, benefits or other support for those who care for a family member with Alzheimer Disease that are at least comparable to benefits that exist to address childcare needs”. While a number of the consultees recognized that employers do not have unlimited resources, consultees also suggested that employers should be willing to accommodate reasonable requests for care leave.
The fact that the significant costs associated with elder care have not been formally recognized by current policies is causing many caregivers some degree of financial hardship...There is a need [to] review related policy to ensure that equal value is placed on elder care as is placed on caring for adults and children with disabilities and to financially assist caregivers to provide the type of support that older care recipients need.
(The Alzheimer Society of Ontario)
A number of concrete recommendations were offered for the manner in which governments can respond to the needs of caregivers in Ontario. The Ottawa-Carleton CCAC emphasized that legislation is required to ensure that persons providing care are supported and not punished. CARP recommended that support for informal caregivers in the form of CPP benefits and retraining programs should be made available. The Alzheimer Society of Ontario emphasized that caregivers should be offered a “caregiver tax-credit” similar to credits available for caregivers of persons with disabilities. Furthermore, extended health benefits, such as those available for dependent children, should be available for dependent adults. Union Culturelle des Franco-Ontariennes told the Commission that guaranteed remuneration should be available to people who stay at home to care for sick family members.
Alternative Care Options
The Commission heard that to relieve caregiver stress, caregivers need a break from their duties. Day programs, respite programs and home care programs were discussed. The Chatham-Kent CCAC noted that day programs and short stay beds are options for caregiver relief but that they often have limited value. They are useful in the sense that they provide caregivers a break, however, such programs can be difficult to access due to issues regarding transportation to and from such programs. With respect to respite care, they told the Commission that many of the forms of respite care are not flexible enough to address the various needs of caregivers. They suggested that respite care in the home often presents a better option for families. The Ontario Association of Senior Citizens’ Organizations told the Commission that universal services, such as long-term care facilities and home care programs, should be in place with adequate funding to ensure that real alternatives to family care are available.
Recommendations for Government & Community Action
28. THAT the Ministry of Labour extend the new leave provisions of the Employment Standards Act, 2000, to smaller workplaces (including those of less than fifty employees).
29. THAT all levels of government and employers consider providing various forms of support to caregivers. Options for consideration include program support (e.g. programs for caregiver relief), financial support (e.g. tax credits) and flexible work options.
Commission Commitments
9. The Commission will develop a policy statement on elder care that identifies the related human rights issues.
10. The Commission will consider complaints where employees, who care for aging or ailing parents, spouses or same-sex partners, face discrimination on the basis of "family status", "marital status" and "same-sex partnership status".
[42] Canada’s Association for the Fifty-Plus (CARP), Putting a Face on Homecare: CARP’s National Forum on Homecare – Focusing on the Informal Caregiver (Toronto: CARP, June 1999), at 2.
[43] Ontario Community Support Association, In 20 Short Years: A Discussion Paper on Demographics and Aging (Toronto: Ontario Community Support Association, February 2001) at 9.
[44] Employment Standards Act, 2000, S.O. 2000, c. 41.
Conclusion
The content of this report confirms that the current approach to human rights issues facing older persons in Ontario is unsustainable. Older persons in this province continue to face a wide variety of barriers that pose a serious affront to their human dignity and to their independence, security, full participation, and fairness. The issues identified in this Report raise significant human rights concerns to which the Commission and broader society must respond. The effects of ageism, when compounded by discrimination on other grounds (disability, gender, sexual orientation, ethnicity, etc.), heighten the need for action.
The Commission intends to take the first steps toward advancing human rights for older Ontarians by implementing the Commission Commitments contained in this Report. The Commission will implement these commitments with the hope that these efforts will serve as a necessary catalyst to change attitudes, policies and practices.
However, many of the recommendations made in this Report can only be addressed by the government and community partners. There is an essential role in this process for other actors to effect change. Therefore, the recommendations offered throughout this Report are an invitation to government, private and the non-profit sectors to take action and to ensure that the human dignity, independence, security, full participation, fairness and ultimately the equality rights of older Ontarians are protected and upheld.
Appendix A: Summary of recommendations for government & community action
- THAT the five principles contained in the National Framework on Aging be integrated in policies and programs of public and private sector organizations.
- THAT all levels of government evaluate laws, policies and programs to ensure that they do not contain age-based assumptions and stereotypes and that they reflect the needs of older persons.
- THAT the Ministry of Education, school boards and schools develop programs and activities that will encourage a better understanding and a more positive perception of older persons. Intergenerational programming between students and older persons is an integral part of such education.
- THAT professional faculties such as medicine, nursing, social work and nutritional sciences should better prepare their graduates to work with older persons in a more supportive manner, without stereotypes and assumptions.
- THAT regulated professions and voluntary professional associations take steps to raise awareness among their membership about ageism and age discrimination and provide continuing education in this area, for example through courses and publications.
- THAT government, the public and private sectors consider the ‘intersectional effect’ of age and gender in policies and programs, especially with respect to the compounded disadvantage experienced by older women.
- THAT the provincial government enact legislation that will set minimum standards for accessibility for persons with disabilities, including older persons.
- THAT government, the public and private sectors consider the ‘intersectional effect’ of age and disability in policies and programs, especially with respect to the compounded disadvantage experienced by older persons with disabilities.
- THAT government, the public and private sectors consider the ‘intersectional effect’ of age and sexual orientation in policies and programs, especially with respect to the compounded disadvantage experienced by older gay, lesbian and bisexual persons.
- THAT health care and social service providers receive training to enable them to appropriately address the needs of older gay, lesbian, bisexual and transgendered persons.
- THAT residential facilities ensure that gay, lesbian, bisexual and transgendered residents are protected from homophobia, and afforded the same rights and recognition of their relationships as other residents.
- THAT health care and other service providers should seek to find ways to deliver services to a range of ethnic, cultural, racial, linguistic and religious groups.
- THAT the Code be amended to eliminate the blanket defence to mandatory retirement at age 65 and to extend protection against age discrimination to workers over 65. This could be done by removing the upper limit of 65 in the definition of “age” in section 10(1). Employers who wish to have age-based retirement policies will be required to demonstrate that the policy is based on bona fide occupational requirements. Laws and programs that require consequential adjustment should also be reviewed.
- THAT, irrespective of whether the Code is amended, employers and unions reconsider the utility and necessity of requiring employees to retire at age 65 and revise their retirement policies and collective agreements to promote flexibility and choice.
- THAT employers take steps to ensure that workplace policies and procedures do not have an adverse effect on older workers. Workplace human rights policies and education programs should address age discrimination and harassment.
- THAT workplaces should be free of ageist assumptions and stereotypes and employers should ensure that older workers are afforded the same opportunities as their younger counterparts. The value of older workers should be recognized.
- THAT municipal, provincial and federal governments should cooperate to develop a strategy for affordable housing for older persons in Ontario. Options for consideration include rent subsidies, shelter allowances and rental cost protections for older persons. The concept of “aging in place” should be a central consideration.
- THAT all levels of government engage in efforts to ensure that the social housing supply in Ontario meets the existing and future needs of older persons and other vulnerable groups.
- THAT THE ONTARIO Building Code Act, 1992 be amended to incorporate the best principles of barrier-free design.
- THAT developers and builders design and implement barrier-free housing that responds to the specific needs of older persons, including those with disabilities.
- THAT medical schools and training centres for health care professionals and others who work with older persons enhance education on the needs of older persons.
- THAT health care institutions, facilities and services be made accessible to all older persons, particularly those with disabilities.
- THAT the government should exercise caution in the use of age-based criteria in health care programs such as assistive devices, prescription drug and dental programs.
- Consistent with the Eldridge decision, that service providers provide sign language interpretation services where necessary to ensure equal access for persons who are Deaf, deafened and hard of hearing.
- THAT the provincial government take further steps to regulate rest and retirement homes. Issues to address might include a Resident’s Bill of Rights and standards for the use of restraints and end-of-life decisions.
- THAT mechanisms currently in place to address other forms of familial abuse should be extended to apply to elder abuse.
- THAT the provincial and municipal governments take steps to support specialized programs, including shelters, for victims of elder abuse.
- THAT the Ministry of Labour extend the new leave provisions of the Employment Standards Act, 2000, to smaller workplaces (including those of less than fifty employees).
- THAT all levels of government and employers consider providing various forms of support to caregivers. Options for consideration include program support (e.g. programs for caregiver relief), financial support (e.g. tax credits) and flexible work options.
Appendix B: Summary of Commission commitments
- The Commission will develop a public policy statement on age discrimination in 2001/2002.
- The Commission will develop and implement a broad public awareness campaign that addresses ageism and age discrimination.
- The Commission will engage in public awareness activities to educate employers and employees about their rights and responsibilities under the Code, to dispel the myths that are often associated with older workers and to encourage employers to view older workers positively.
- The Commission will develop a discussion paper on housing and human rights that will address issues facing older persons.
- The Commission will communicate with the Ontario College of Physicians and Surgeons, the Ontario Medical Association and the Canadian Medical Association and other appropriate organizations to advise that unequal access to medical treatment and other health care services on the basis of age or disability may constitute discrimination.
- The Commission will contact and meet with professional faculties such as medicine, nursing, dentistry, nutritional sciences and social work to discuss the urgent need to include comprehensive education on age discrimination within their curricula and to ascertain their plans for including such education in their programs.
- The Commission will continue to take steps to promote accessibility amongst service providers throughout Ontario.
- The Commission will continue to monitor the outcomes of the provincial plan of the Round Table for Ontario’s Elder Abuse Strategy that are within its mandate.
- The Commission will develop a policy statement on elder care that identifies the related human rights issues.
- The Commission will consider complaints where employees, who care for aging or ailing parents, spouses or same-sex partners, face discrimination on the basis of "family status", "marital status" and "same-sex partnership status".
Appendix C: Organizations that provided input
Advocacy Centre for the Elderly
AIDS Committee of Toronto
Alzheimer Society of Ontario
ARCH (Advocacy Resource Centre for the Handicapped)
Award Personnel
C.A.R.P. (Canada’s Association for the Fifty-Plus)
Canada Mortgage and Housing Corporation
Canadian Centre for Activity and Aging
Canadian Hearing Society (London)
Canadian Hearing Society (Toronto)
Canadian Hearing Society (Ottawa)
Canadian Hearing Society (Sudbury)
Canadian Manufacturers and Exporters (Ontario Division)
Canadian Mental Health Association – Windsor Essex
Canadian Pensioners Concerned
C.A.W. (Canadian Auto Workers)
Chatham/Kent Community Care Access Centre
City of Toronto Homes for the Aged Division
Community Care Access Centre of Halton
Community Care Access Centre Timiskaming
Council on Aging – Frontenac/Kingston
Council on Aging – Ottawa-Carleton
Council on Aging for Renfrew County
Dieticians of Canada
Faculty Group: Carleton University
Finnish Social Counselling Service of Toronto Inc.
Golden Years Club
Halton Health Department, Community Health Services Department
Halton Region’s Elderly Services Advisory Committee (ESAC)
Kingston, Frontenac, Lennox & Addington Community Care Access Centre
Ministry of Health and Long-Term Care
Ministry of Labour
Ministry of Municipal Affairs and Housing
Muskoka, Nipissing, Parry Sound Local Training and Adjustment Board
National Anti-Poverty Organization
Northwestern Ontario District Health Council
Nova Scotia Human Rights Commission
Older Women’s Network
Ontario Association of Non-Profit Homes and Services for Seniors
Ontario Association of Social Workers
Ontario Coalition of Senior Citizens’ Organizations
Ottawa Carleton Community Care Access Centre
Over 55 (London) Inc.
Phone Busters (Ontario Provincial Police)
Registered Practical Nurses Association of Ontario
Scarborough Community Care Access Centre
Senior Link
Steering Committee on Social Justice
The Alliance of Seniors to Protect Canada’s Social Programs
The Canadian Association of the Deaf
The Coalition of Lesbian and Gay Rights in Ontario
The Fair Rental Policy Organization of Ontario
The Toronto Board of Trade
Union culturelle des Franco-Ontariennes
United Generations Ontario
United Senior Citizens of Ontario
A number of individuals also provided comment during the consultation. To protect their privacy, the Commission has chosen not to list their names. The Commission is very grateful for their input.